
Note: This was a 2-part series (Part 1 & 2) that we merged together. The concluding article (Part 3) can be found here: Cholesterol: Myths & Misconceptions.
Cholesterol is a substance that plays many essential roles in the body. It is involved in things like the structure of our cells, brain and nerve function, and hormone production. It is so important that every cell in our body can make all the cholesterol it needs without relying on high amounts to be delivered from the blood. Babies born without the ability to make their own cholesterol have severe birth defects and can die as a result. We can also consume cholesterol in certain foods derived from animals. It is frequently described as a fatty or “waxy” substance. While different from body fat, cholesterol and body fat are in the same family of substances collectively known as “lipids”.
One important characteristic of lipids, including cholesterol, is that they do not dissolve in water. This is due to their chemical structure. Think of when you try to mix oil and water – they really don’t like one another and will separate on their own. Because humans are mostly made of water, cholesterol won’t dissolve in the blood and needs help getting around. We have special carriers called “lipoproteins” to pick up things like cholesterol and other lipid substances that don’t like water to help them move through the bloodstream.
In this article series we will cover the basics of cholesterol and why we should care about it, what to do when it is high, and address a variety of related myths and misconceptions.
Why do we care about cholesterol?
We have known for a very long time that cholesterol in the blood is related to the risk of heart attacks and strokes. But the relationship between cholesterol and heart disease is complicated. For example, there are people who suffer heart attacks who do not have extremely high cholesterol levels. There are other people who have low cholesterol levels who die prematurely. This has created a lot of confusion and arguments about how important cholesterol really is and how concerned with it we should be. The short answer is that it is important and healthcare professionals are rightly focused on it, despite what many claim. We will explain these apparent contradictions and clarify areas of confusion throughout this article series.
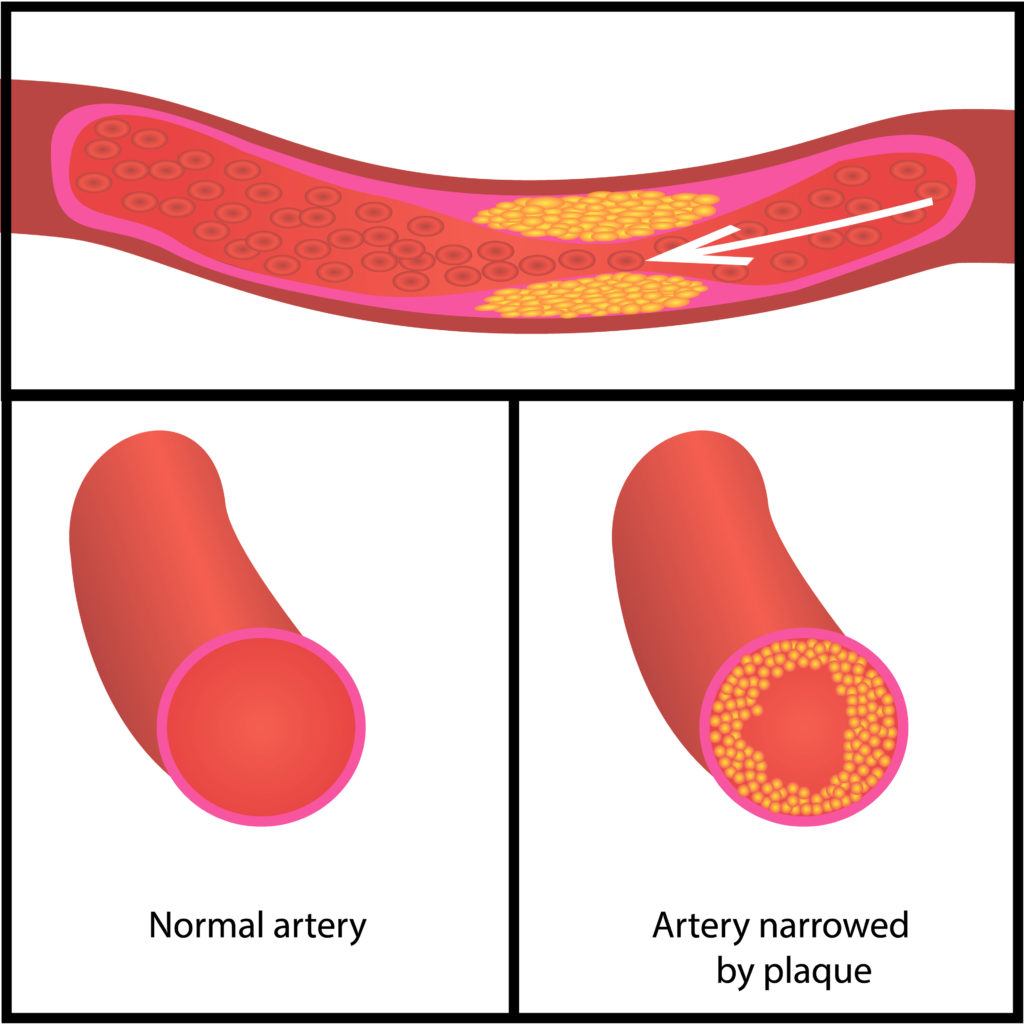
Lipoproteins come in a variety of sizes, but many of them are extremely tiny – smaller than 70 nanometers in size, or 0.00000007 meters. Particles this small can penetrate the walls of our blood vessels. When this happens, they deposit their cholesterol and this causes inflammation in the vessel wall. These collections of cholesterol and inflammation are called “plaques”. Plaques can grow over time and limit blood flow through our vessels. They can also break loose and cause sudden blood clots that stop blood flow to important organs, resulting in problems like heart attacks and strokes.
When blood cholesterol levels are high for a long time, the tiny lipoproteins have more opportunity to get into our blood vessel walls and cause problems. Heart disease risk is related to how high these levels are, but more importantly how long they are elevated over the course of your whole life. [Robinson 2018] This is why many heart attacks and strokes occur in older people who have had decades of exposure to milder elevations in blood cholesterol, but it is also possible for people with extremely high levels to have these problems earlier in life too. In fact, about 40% of these events happen in people younger than 65 years.
However, risk is not “all-or-nothing”. In the same way that not everyone who smokes throughout their life will develop lung cancer, some people with higher cholesterol levels may not experience a heart attack. Regardless, the risk is still present, depending on the total levels over the entire lifespan. The earlier in life we get blood cholesterol levels under control, the lower the risk of heart disease in older age. On the other hand, waiting until old age to start treating patients for high cholesterol has much smaller benefit, since a lot of the damage has already been done.
Blood cholesterol levels are not the only contributor to heart disease and strokes. Other things like smoking, high blood pressure, diabetes, and inflammation are very important too and will be covered in separate articles. But even when people do not have any inflammation, have normal blood pressure and blood sugar, and do not smoke, higher blood cholesterol still increases the risk of heart disease compared with lower cholesterol. [Yusuf 2004] [Friera 2017] Fortunately we have learned about lots of things that influence blood cholesterol levels and heart disease risk. This has led to many effective treatments and a massive decrease in heart disease deaths since the mid-20th Century.
How is high cholesterol diagnosed?
Most people who see a primary care doctor will have a cholesterol test done at some point. Recall that there are many things that do not dissolve in water that need to be carried around the blood on lipoproteins. A cholesterol test measures how much of these are in the blood.
- Total cholesterol (TC): this tells you total amount of cholesterol being carried on all lipoproteins.
- High-Density Lipoprotein-Cholesterol (HDL-C): this tells you the amount of cholesterol being carried on a specific lipoprotein called “HDL”. This is often called “good” because having higher levels of HDL-C is associated with less heart disease. Unfortunately this is just a correlation – not a causal relationship, which is why research has shown that doing things to increase this level does not help.
- Triglycerides (TG): these are a form of fat that is carried on lipoproteins. Lipoproteins deliver triglycerides to our organs and tissues, where they are burned for energy. While an important contributor to heart disease risk on their own, we will spend less time on them in this article. Extremely high levels (greater than 500 mg/dL) require aggressive medical treatment to prevent other complications. Otherwise, follow the remaining discussion.
- Low-Density Lipoprotein-Cholesterol (LDL-C): this tells you the amount of cholesterol being carried on a specific lipoprotein called “LDL”. This is often called “bad” because LDL is the main – although not the only – lipoprotein that gets into blood vessel walls, depositing cholesterol and setting off the inflammation that causes plaque to grow. There is some variation in the size of LDL particles, but all of them – large or small – typically range from 20-30 nanometers in size, much smaller than the 70-nanometer threshold to get into the walls of our blood vessels and cause trouble.
We can see that there are multiple different components of a standard cholesterol test. If someone is told they have “high cholesterol”, which numbers are we talking about? Let’s try to simplify.
By taking the total cholesterol (TC) and subtracting the high-density lipoprotein cholesterol (HDL-C), we obtain a number known as non-HDL cholesterol (non-HDL-C). Subtracting the “good” stuff from the total amount leaves us with an estimate of all the “bad” stuff; that is, all cholesterol being carried on lipoproteins that can be harmful. For example, consider the following blood test results:
- Total Cholesterol: 200 mg/dL
- High-Density Lipoprotein Cholesterol (HDL-C): 50 mg/dL
- Triglycerides: 110 mg/dL
- Low-Density Lipoprotein Cholesterol (LDL-C): 120 mg/dL
Simple math shows a non-HDL cholesterol of 200 – 50 = 150 mg/dL. This number gives us a better predictor of heart disease risk from a regular cholesterol test than LDL-cholesterol alone. For individuals who are generally healthy, a non-HDL cholesterol less than 130 mg/dL is a reasonable goal. There is further benefit at even lower levels, and there is no blood level that is “too low”. Recall that our cells can make all the cholesterol that they need for themselves, without relying on high levels to be delivered from the blood.
For individuals who are at high risk for heart disease (for example, those with certain genetic conditions or who have already had heart disease problems like a heart attack), the goal is to get this non-HDL cholesterol level as low as possible. A particularly risky situation is when the cholesterol panel shows a high LDL-C, a high triglyceride level, and low HDL-C. This is often seen in people with diabetes and other conditions that significantly increase the risk of heart disease.
An even better test involves measuring the actual number of lipoproteins rather than the amount of cholesterol they carry, as is done on the basic cholesterol test. This is called an Apolipoprotein B measurement, abbreviated as ApoB. It provides a superior measure of heart disease risk, but many doctors are still unfamiliar with it and may be reluctant to order it. [Sniderman 2021] Hopefully this changes in the future, since it is not a very complex or expensive blood test to perform and provides even better information.
There is a lot more to interpreting blood cholesterol tests but we will use this approach for now. There are many other tests that can be performed beyond the basic cholesterol panel and apolipoprotein B measurement, but most of them do not provide much added value for predicting risk beyond what has been discussed here.
Factors that Influence Cholesterol Levels
Genetics
Genetics have a major influence on blood cholesterol levels. Sometimes a variation in a single gene inherited from our parents can cause high cholesterol by itself, whereas in other situations the elevation can result from the effects of multiple different genes. A low-density lipoprotein cholesterol (LDL-C) level over 190 mg/dL raises suspicion for (although does not guarantee) a type of genetic cause known as “Familial Hypercholesterolemia.” Inherited genetic causes of high cholesterol can result in extremely high cholesterol levels from birth, but milder elevations often have genetic contributions too. These people can experience accelerated plaque development and heart disease complications even without other risk factors like inflammation, diabetes, obesity, high blood pressure, or smoking.
Since we cannot easily change our genes, people with genetically high cholesterol are typically unable to get their blood levels controlled through diet or exercise alone. This is not their fault, nor is it due to a lack of effort or willpower – it is simply the genetics they inherited. This also does not mean that people with genetic issues shouldn’t work on the lifestyle factors we will discuss next, but that these efforts may not be enough to get them all the way to a low risk level.
The risk of developing heart disease is related to how high blood levels are, and how long they are elevated over the entire lifespan. This means that it is even more important for people with genetically very high cholesterol to get it under control, since they were likely born with high levels that went undetected and untreated for many years before their first blood test, often as an adult.
For people who seem to be doing everything “right” from a lifestyle standpoint and cannot get their blood cholesterol into a low risk range, genetic issues are likely to be a major factor. Medications are typically necessary to lower the risk of disease in these situations and should be discussed with a doctor. There is ongoing research into gene-editing treatments that may provide easier long-term treatment for these issues in the future.
Diet
Diet is the most significant lifestyle behavior that affects blood cholesterol levels. There are many ways the foods we eat can influence our blood cholesterol and overall disease risk. The two main targets we will focus on for this article are fiber and the types of fat in the diet.
Eating high-fiber foods is an excellent way to lower blood cholesterol levels. We recommend all people eat at least 30 grams per day of fiber from their food. This includes sources like fruits, vegetables, legumes (like lentils, beans, and chickpeas), and whole-grain sources like oats and barley. The more fiber someone consumes, the more blood cholesterol levels tend to decrease – so if someone is willing to eat much more than 30 grams per day from their food, they are encouraged to do so. Replacing highly processed, packaged, often sugary foods with these options can have enormous health benefits beyond cholesterol too. These include lowering blood pressure, triglycerides, lowering colon cancer risk, and promoting weight loss by increasing feelings of fullness.
The other major factor is the type of fat in our habitual diet. There are many kinds of fat in our food. You may have heard of “healthy fats” and “unhealthy fats”, or seen a Nutrition Facts label listing “saturated” and “polyunsaturated” fat. These all have different chemical structures leading to unique effects on our health, and some tend to be better than others.
Consuming high amounts of saturated fat from animal food sources (such as butter, lard, and fatty red meat) tends to increase cholesterol and disease risk, particularly when saturated fat calories start to exceed 18-20% of total calories. People don’t need to track this exact quantity in their daily life, but it is worth pointing out because this is a consistent finding in the research.
Replacing a significant portion of animal-derived saturated fats with unsaturated fats from fish (like salmon), nuts (like walnuts and almonds), avocados, olive or canola oil, or other plant sources results in large decreases in blood cholesterol and disease risk. Replacing these saturated fats with high-fiber carbohydrate sources is also beneficial, but has a less potent effect than replacement with unsaturated fats from the types of foods listed above. Li 2015
The specific ways these types of fats influence blood cholesterol levels are beyond what we will address here, but we have decades of controlled feeding studies consistently showing these effects in humans. Clarke 1997 Note that this does not mean one should never eat any animal food sources containing saturated fats. Rather, these foods should not form a large part of the habitual diet. They should be restricted more aggressively for those known to have extremely high blood cholesterol levels or known heart disease.
You may be surprised that we do not place a lot of emphasis on the total amount of fat or cholesterol in the diet. This is because these factors are less significant compared to the types of fats that are eaten on a regular basis. It is possible to consume a lower-carbohydrate, higher-fat diet without causing cholesterol or heart disease problems, if the diet still contains plenty of fiber and the fats are primarily unsaturated from fish, nuts, and other plant sources. There are some people who may need to lower their intake of cholesterol in the diet, but we recommend focusing on these more important factors first.
The same general dietary modifications are recommended for individuals with significantly high triglycerides. We often inquire about the amount of refined carbohydrates in the habitual diet (things like sugar-sweetened drinks and foods, baked goods, processed snack foods, etc.) and aim to replace these with the more healthful options described above. If an individual is carrying excess body fat (see next item below), this is another important factor to address high triglycerides as well. There are also genetic conditions that can cause high triglycerides on their own.
Body Fat
Body fat can have a significant impact on our blood cholesterol levels by interfering with liver and hormone function that is important for cholesterol regulation. We can easily determine whether we have excess body fat using a simple waist circumference measurement. We have a specific article and video showing how to do this.
If a person has too much body fat, aiming to decrease it to healthy levels can have significant health benefits, including decreasing blood cholesterol levels. The details of weight loss strategies are beyond the scope of this article, but meeting or exceeding current physical activity guidelines is one important aspect of the process, along with changes in the overall dietary pattern. We have mentioned some of the recommended dietary changes to improve blood cholesterol above, and physical activity can also help improve general health and blood cholesterol levels in numerous other ways.
The process of decreasing body fat levels is complex and challenging for many people, since it is very heavily influenced by genetics and our surrounding environment. Some may be able to achieve healthy body fat levels relatively easily through diet and exercise alone, whereas others may need additional help with the use of medications or surgical treatments like gastric bypass surgery. It is important to reduce the stigma around obesity, and around the use of medications or surgery to treat it just like any other disease.
Decreasing waist measurements to the “healthy” range for your demographic is a strong recommendation for people with high cholesterol or other health problems related to excess body fat.
Other Medical Issues
If a person is diagnosed with high cholesterol, thyroid function should be checked since thyroid hormone plays an important role in cholesterol regulation. The thyroid is a gland in the neck that controls several essential body functions. If someone has high cholesterol levels and they are found to have low thyroid function (hypothyroidism), treating the thyroid issue can help bring the cholesterol levels back down. This is a less common scenario compared with the other issues discussed so far, as hypothyroidism is estimated to occur in approximately 1.4-13% of patients with high cholesterol, but it is simple enough that it should not be overlooked. Tagami 2011
Finally, certain medications can also result in high cholesterol blood levels. It is worth asking your doctor if any of the prescription medications you are taking could be contributing, and whether the benefits of taking those medicines outweigh the risks for your situation. Sometimes there are alternatives without these side effects, whereas in other situations this may not be an option. Anabolic steroids often negatively influence blood cholesterol levels and are not recommended.
What Comes Next?
Once high cholesterol or existing heart disease are diagnosed, the next steps involve using all available information to estimate your future risk of heart disease complications. While current guidelines recommend using tools to estimate your 10-year risk of heart disease complications, we feel this is a shortsighted approach, particularly for younger people who should expect to live much longer. Some experts have proposed using a 30-year risk estimate to guide treatment decisions, since the risk of heart disease complications is related to the cumulative, life-long exposure to lipoproteins in the blood. Thanassoulis 2018
For people who have low overall risk and mildly elevated blood cholesterol, focusing on the lifestyle behaviors discussed above may be enough to achieve the goal blood levels. To review, these include:
- Replacing high intakes of animal-derived saturated fats (like butter and fatty red meats) with unsaturated fats from fish (like salmon), nuts, and other plant sources
- Increasing dietary fiber from fruits, vegetables, legumes (like lentils), and other whole-grain sources (like oats) to a minimum of 30 grams per day, but even higher intakes provide additional benefit
- Reducing waist circumference to a low risk range for your demographic through changes in dietary habits, regular exercise, and potentially the use of medications or surgery in consultation with a physician
We do not necessarily recommend a diet low in overall fat in this situation, instead placing more emphasis on the types of fats in the habitual diet. We also do not recommend aggressively limiting dietary cholesterol as a first intervention since this tends to have little effect on blood cholesterol levels, particularly when the types of fats in the habitual diet are improved. After making these lifestyle changes, it is reasonable to re-check a blood cholesterol and/or apolipoprotein B test in 2-4 months.
We do not recommend any specific interventions to raise high-density lipoprotein cholesterol (HDL-C, the “good” stuff) even though it is associated with less heart disease. This is because studies on treatments that raise HDL-C levels have not shown benefits. Additionally, studies of genetic variations in HDL-C levels have not found any direct impact on heart disease risk. Voight 2012 This suggests that HDL-C is not a causal contributor to heart disease, but is rather an associated marker. In other words, healthier people tend to have higher HDL-C levels, less healthy people tend to have lower HDL-C levels, and directly changing this blood level does not have any direct impact on heart disease risk. This contrasts with low-density lipoprotein (LDL), which has evidence that treatments to reduce LDL-C levels also reduce heart disease risk, as well as studies of genetic variations in LDL-C levels that find direct impacts on heart disease risk.
For people with persistently high blood cholesterol (or who are otherwise at high risk), we may recommend use of medications in addition to the above lifestyle behaviors. Ultimately, the goal is to achieve the largest long-term decrease in risk of heart disease complications – and the earlier in we can achieve good control of blood cholesterol, the better. Discussion of specific medications is outside the scope of this article and should be discussed with your doctor. Fortunately, there are many safe options that can effectively reduce these risks. Remember that it is OK to benefit from medicines, especially if you are at high risk. No one wins a prize for avoiding the use of medicines and living at higher risk than necessary, especially if it leads to a preventable heart attack down the road.
In addition to what has been discussed so far regarding blood cholesterol, other contributors to heart disease and stroke risk should be addressed. This includes things like blood pressure, smoking, alcohol use, and other diseases that may be present that can influence heart disease risk. The specifics of these topics are beyond the scope of this article and will be discussed elsewhere.
This should provide a general overview of what cholesterol is and why it is an important factor in heart disease. It should also provide a roadmap for things you can do about it, if yours is elevated. Cholesterol is not the only thing to worry about when it comes to heart disease risk, but high blood levels very clearly increase our risk for serious health problems. This is not unfounded advice based on outdated data. In fact, the base of scientific evidence on this topic has only strengthened over time, conclusively demonstrating that having long-term elevations in blood cholesterol is not good for us. Diet and exercise are important for reducing risk, but there are also factors like genetics that are outside of our control. As a result, medications can play a critically important role in some cases upon the advice of a physician. Next, we will finish this series by addressing common myths and misconceptions about blood cholesterol as it relates to heart disease risk.
Thank you to Tom Campitelli, DTFP, for his assistance in editing this article.