So you’re experiencing pain in your heel. It’s especially painful when you take your first few steps out of bed in the morning and limits your usual activities. This article will explain what is going on, why it may have developed, and what you can do to feel better. We will provide actionable steps to manage typical heel pain, and provide options that athletes can use to continue training and increase their tolerance for activity.
What is it?
Common names for this condition include plantar fasciitis or plantar fasciopathy. This pain affects the bottom of the foot, known as the “plantar” side, and specifically involves a sheet of connective tissue running along the length of the foot known as the “plantar fascia”. The pain is typically located at the base of the heel. “Fasciitis” implies an inflammatory problem, whereas “fasciopathy” encompasses a broader set of contributors to pain in the area. For the rest of this piece, we will simply refer to it as plantar heel pain. Note that this is a different condition from pain affecting the Achilles tendon or other areas of the foot, even though plantar heel pain has many similarities to tendinopathy.
The condition often involves pain with walking, especially after a prolonged period of inactivity. A typical experience is significant pain upon the first few steps after getting out of bed in the morning, followed by a gradual improvement with movement throughout the day.
Plantar heel pain is typically diagnosed based on the description of symptoms and by palpation. In other words, “it hurts when the area is poked.” Imaging tests like X-rays or CT scans are typically not needed in cases where there has not been any traumatic impact or direct injury to the heel. While some recommend the use of ultrasound for diagnosis, there are issues with this since many supposedly abnormal ultrasound findings, like “increased signal”, can also be seen in people with no heel pain or as part of the normal adaptive process to exercise. Radwan 2016 Dasi 2022 This makes the presence of such findings less helpful in confirming a diagnosis using ultrasound compared with the person’s description of symptoms and examining the area.
What contributes to Plantar Heel Pain?
Factors that contribute to this kind of heel pain include having a body mass index greater than 27, excessive running, a sedentary lifestyle, and jobs requiring prolonged standing or walking.
So, as with other pain issues we’ve discussed before, we are dealing with a problem of excessive loading. However, “excessive” is unique to the individual and depends upon their usual activity habits. For example, an ultra-marathoner is likely just getting warmed up at the weekly mileage of a recreational 5k runner, whereas someone who is generally sedentary may exceed their capacity simply by walking around a mall or visiting a theme park for a day. This sudden change in training or activity is more often the driving factor than the absolute amount of activity; in other words, it often results from doing too much, too soon.
A variety of biomechanical factors are often blamed for this condition. For example, limited ankle dorsiflexion is often cited as a contributing factor. This describes a limited ability to bend the foot upwards and draw the toes up towards the shins. More recent studies have not found this to be a strong contributing factor to plantar heel pain.
What can you do about it?
The good news is that most cases get better on their own over the course of a year. But most people do not want to wait that long and are looking for immediate pain relief. A search of the internet, or even the scientific literature, often does more to confuse than to set a clear path forward for what to do about this condition. Everything from custom orthotics and other passive treatments to injections and aggressive surgeries are offered, even though most don’t have strong evidence that they actually work.
We will take a pragmatic approach to this condition, as it does have simple steps that, if addressed, can decrease pain and allow for a return to activity.
Step 1: Assessing and adjusting for recent changes in load
Plantar heel pain symptoms are often accompanied by a recent increase in training or daily activities such as standing or walking. If this is the case, it is beneficial to make adjustments to your level of activity until you have adapted. Recently increasing your mileage running, abruptly changing shoe type, or going on a vacation that involves more standing, walking, or hiking can all contribute to symptoms. See if you can make smaller adjustments in the overall amount of workload placed on the feet, or consider whether some of the changes may have been transient (as with a vacation), and can be expected to improve on their own.
If symptoms are more related to a recent change in job or work demands such as having to stand for longer periods of time, this may not be as easy to modify if it’s required for the work. In these situations additional steps may be necessary.
Step 2: Strengthening the foot and ankle
The focus of the exercises offered here is for short-term pain management, since changing the structure of tissues necessarily takes time. The initial relief from focused exercises may just result from loading the area in different ways than you are used to. There is evidence from multiple studies that a stretch for the plantar fascia and calf muscles can provide short-term relief. The studies typically have people hold the stretches for 10 seconds, for 10 repetitions. Strengthening exercises for the foot and ankles appear to be effective as well.
We want to be clear here that the plantar fascia is a thick, fibrous tissue and stretching of any capacity is unlikely to change actual tissue length. It is being done for relief of pain symptoms more than it is for the expectation of “lengthening” the tissue.

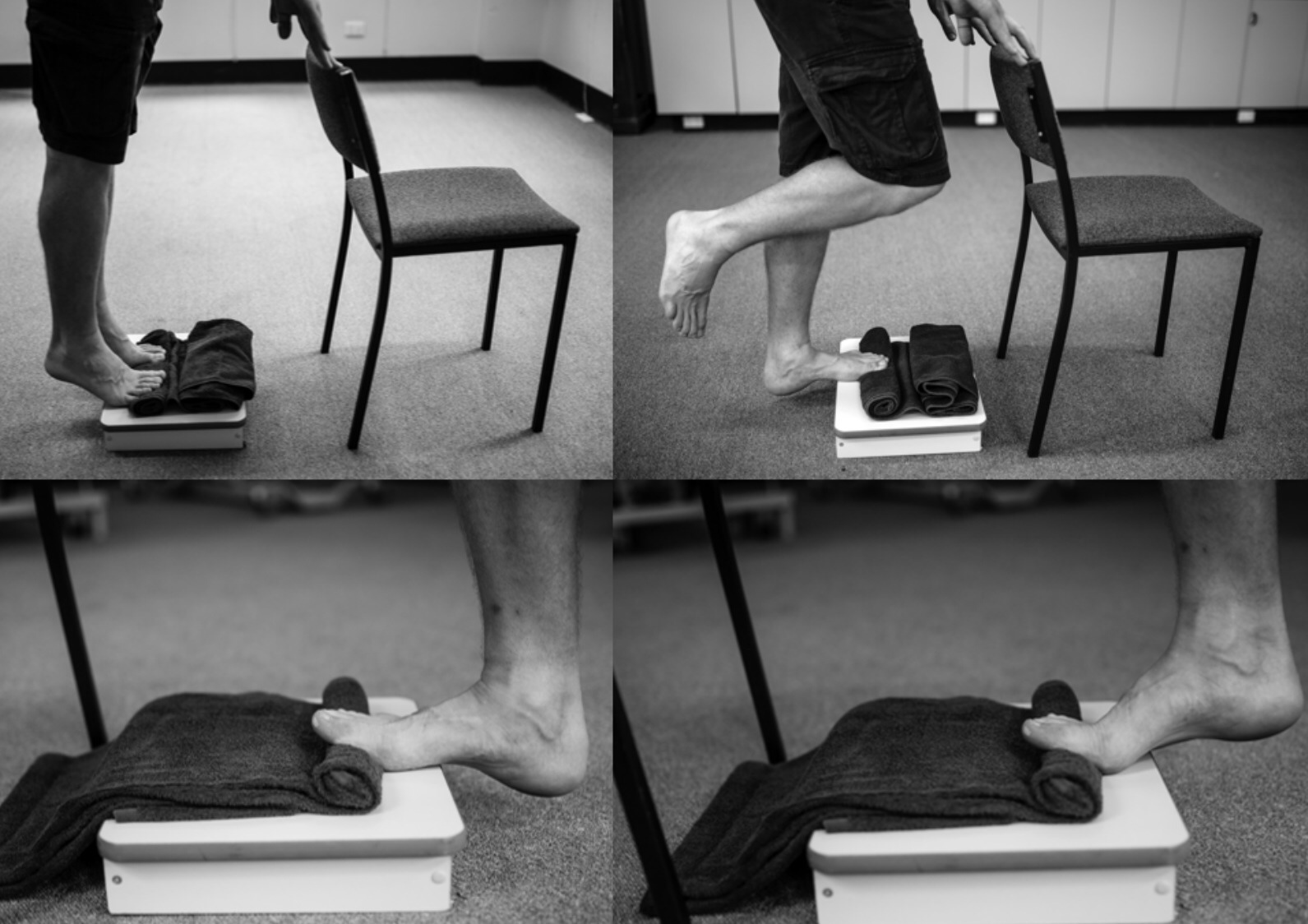
Strengthening the foot and ankle involves performing calf raises with technique that places tension on the plantar fascia. This can be done by performing calf raises with a small towel rolled up and placed under the toes. Athletes can start with a double-leg version for 2-3 sets of 15 repetitions, then progress to a single-leg version.
Other exercises using external load such as a soleus raise, seated calf raise, calf raises on a leg press, or a “donkey calf raise” can all play a role as well. Plantar heel pain symptoms are often related to the load placed on the area; for an especially strong athlete who has increased overall training volume, bodyweight calf raises alone may not provide enough intensity to address the issue. For the barbell athlete, we recommend selecting 1-2 calf-specific exercises to be performed twice per week while in the gym once the athlete has progressed beyond the bodyweight exercises mentioned above.

Single-leg exercises can also be performed that challenge both strength and balance. We recommend exercises such as a curtsy lunge, single leg deadlift, or lunges as a means of challenging the foot and ankle in a new and different way. Begin with either light weight or bodyweight alone, to place the initial emphasis on balance and control over strengthening in the traditional sense. The immediate goal is not to increase the load, but rather to improve balance while performing these movements. While most Barbell Medicine readers come from a resistance training background, exercises that push a broader athletic spectrum can be beneficial to challenge a person in different ways.
A sample program is provided at the end of the article below.
Step 3: Footwear and orthotics
While load management and exercises are the first-line steps for plantar heel pain, some athletes may continue to experience pain and need other strategies for relief. Footwear options are a common question in the setting of plantar heel pain.
There is no evidence that any particular shoe is better than another, or that custom orthotics are absolutely necessary to treat this condition. Using an orthotic insert or a different shoe for plantar heel pain just provides another way to modify load on the affected area. Orthotics can be beneficial for short-term relief of symptoms, but orthotics are a temporary modification and do not need to be worn forever if activity and loading is appropriately managed and progressed over time. If you choose to use an orthotic, we suggest a simple over-the-counter version rather than an expensive “custom” version.
As for shoes, if an athlete has recently switched from a rigid shoe to a “minimalist” shoe or vice versa, they might consider alternating between pairs as they adjust to the new change. Anecdotally, individuals with heel pain tend to feel better in a more rigid shoe when experiencing a lot of pain. This is a viable option if the goal is short-term relief, but once again should not be viewed as a permanent solution. We adapt to the stresses to which we are exposed, and while temporarily changing a pattern can be beneficial, it does not allow for long-term adaptations.
Step 4: The Other Stuff
There will always be some treatment du jour when it comes to musculoskeletal injuries, and you can find people looking at everything from magnetized insoles to wheatgrass cream. None of these have demonstrated a benefit beyond placebo and we do not recommend them. There are also a host of injections ranging from corticosteroids, botox, platelet rich plasma and even dry needling where you get poked without any medication. None of these interventions have demonstrated anything beyond small effects for short-term pain relief with no substance proving superior to the other. The risk of harmful adverse events with injections also cannot be overlooked. In general, we do not recommend injections or dry needling for the treatment of plantar heel pain.
Low level evidence does exist for extracorporeal shockwave therapy but there are conflicting results from other meta-analyses. If an individual is participating in exercise and other conservative measures and not getting relief, this can be tried alongside the measures we’ve already discussed, but is not a first-line treatment.
The Big Picture
Let’s summarize the actionable steps that you can take to manage symptoms, and continue to train while dealing with heel pain.
- Manage load: If there have been any recent changes in activity, try to control for dramatic increases where you can. “Excessive” activity is relative to the person and there are numerous ways that you can increase capacity for training. That being said, if there is a recent increase due to constraints at work, we may need to seek other means to address pain issues.
- Specific training modifications: Isolated foot and ankle strengthening can be beneficial for managing symptoms and building capacity for loading long-term. Performing calf raises with a foot bias, stretching the bottom of your foot, and incorporating single-leg exercises can all provide a different stimulus to help manage symptoms.
- Footwear changes: An athlete may benefit short-term from using an over the counter orthotic or more rigid shoe. There is no need for a custom orthotic, long-term use of an orthotic, or for a specific brand/type of footwear. However, shoes that support the foot more and limit great toe dorsiflexion (“pulling your big toe up”) are often tolerated better. This is a compensatory strategy though, and other modifications need to be addressed to restore normal function long-term. Finding a shoe that is comfortable for you is more important than trying to find the perfect shoe based on someone else’s opinion.
- The “other stuff”: There is no good evidence for passive modalities such as instrument-assisted soft tissue massage, dry needling, or kinesiotaping. It can feel good to rub on areas that hurt, but the specificity of the technique does not matter and it is not helping the area adapt and restore normal function. Your plantar fascia is thick, springy, fibrous tissue meant to support your entire weight. The narratives associated with many of these techniques are unsubstantiated; for example, practitioners who perform aggressive massages of the area are not “breaking up adhesions” or “releasing tissue”. The evidence for injections of any type is not strong and we would not recommend this form of treatment in most situations. Part of the issue here is that most treatments are non-standardized, and the claims associated with them are not matched by the research supporting them.
- Expectations: The major upside of plantar heel pain is that most often it will resolve on its own, but this does take time. When you cannot do everything you want to do sometimes it is hard to see the progress you have made. It can be helpful to turn one of the problematic tasks into quantitative goals so you can see progress. If standing for 30 minutes causes pain and your goal is to stand for 2 hours, increasing the amount of time you can stand to 45 minutes is still short of the goal but you have improved your overall time by 50%, which is significant. Being able to see these gains can help frame progress to see the small wins over time.
Sample Program
This is by no means comprehensive, but can serve as a starting point for pain management. The program can be done 2-3x/week as part of normal training with the plantar fascia stretch performed as-needed throughout the day for 4-5 sets of 10 second holds.
Plantar fascia-biased calf raises (starting double-leg and progressing to single-leg as tolerated)
3 sets to 2 reps in reserve
Once you can achieve 15 repetitions double-leg for 3 sets, it is time to progress to single-leg
Single-leg deadlift
3 sets of 8 reps with a light weight (starting cap 25 lbs) working on balance and control
Curtsy lunge
3 sets of 8 reps with a light weight (starting cap 25 lbs) working on reaching as far as you can control
Note: You can substitute out different single leg exercises here, as these are a suggestion. For these exercises the emphasis is on control over absolute weight. Progressing into single-leg lunge variants can be a good next step, as this movement does emphasize more great toe extension.
For a barbell athlete or someone experiencing symptoms with daily activities who is not very active, the above set-up provides a good starting point. For athletes whose sport and activity has an explosive power component (e.g., jumping) it is beneficial to perform drills as part of the later rehab phases to re-introduce power before returning to normal sport activities. This can involve exercises like bounding drills, pogo hops, or various other sport-specific movements.
If you have tried this advice and are still experiencing symptoms, it can be beneficial to consult with our Pain and Rehabilitation team to find an entry point and progression plan for your training.