
The efficacy of placebo in enhancing performance is as well established as it is multifactorial. Geers 2014 This presents a paradox of a placebo being an inert substance, yet still having an effect on performance. A movement has recently transpired to move away from the term “placebo effect” and toward “contextual factors” to address apparent paradox.Rossetini 2018 Contextual factors have been implicated in the effects of ergogenic aids, anabolic steroids, creatine monohydrate, and a variety of other substances and devices. Beedie 2009 Oral placebos have consistently shown approximately 2% increases in moderately trained endurance athletes. Beedie 2006, McClung 2007 The effect of the placebo has shown even greater effects when administered by an injection/needle. Zhang 2008
Key Points:
- Trained runners given a placebo that they perceived as an active drug were able to improve their 3 km running performance by almost 10 seconds versus a control group only improving 2 seconds.
- The placebo, according to participants, reduced the qualitative perception of effort and increased motivation without changing the quantitative perception of effort via rate of perceived exertion.
- An inert substance was able to increase performance without changing heart rate, rate of perceived exertion, or hematological variables, alluding to the role that beliefs play in performance.
Athletes are constantly in search of anything that will give them a competitive edge, with the complementary health industry in American generating $30 billion dollars/year .Nahin 2012 The vast majority of those supplements, treatments, and advice completely lack evidence of efficacy, and of those that do, most are illegal in higher levels of competition. Over the past two decades, the use of performance enhancing drugs (PEDs) has been on the rise.Carpenter 2007, Stano Rossi 2011 Specific to endurance athletes, one of the most popular drugs is recombinant Human Erythropoietin (r-HuEPO) which has been shown to increase hematocrit (Hct).Durussel 2013 Even here, the effect on physiological changes translating to increased performance is in question, but the drug is now synonymous with the sport of cycling. Heuberger 2013
The association of r-HuEPO with increased performance can serve as an anchor with which to prime athlete expectations. Tversky 1974 The expectation being that taking a substance with the same effects of r-HuEPO should increase performance as well. A 2015 study aimed to explore the magnitude of those effects on performance of an injected placebo made from saline that they called “OxyRBX.” Let’s review this study more closely to see what they found.
Study Design
The purpose of this study was to quantify the effect of a placebo injection purported to have the same level of effect as a proven drug (r-HuEPO) on endurance running performance in a field based, head-to-head competition.
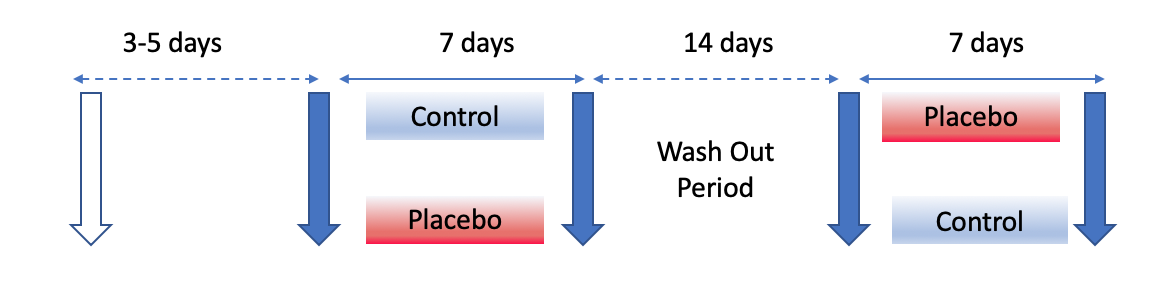
This was a randomized cross-over design, with participants undergoing tests before and after a 7-day “control” phase during which no intervention was given, and a 7-day “placebo” phase during which individuals were administered daily subcutaneous saline injections (0.5mL of 0.9% NaCl) that they thought to be OxyRBX.
The study recruited 19 endurance-trained males, with three dropping out prior to the study due to concerns of possible complications. One additional participant dropped out without giving a reason. This left 15 well-trained club level athletes who engaged in 213 +/- 129 minutes of endurance training and 50 +/- 58 minutes of resistance training per week. Their personal record (PR) in a 10-km race was 39.3 +/- 4.4 minutes.
Participants were given an informed written consent that they were taking a “legal erythropoietin-like substance, OxyRBX,” to enhance deception. After the study all participants were debriefed that they had taken a placebo. Prior to the study all participants were informed of the effects of r-HuEPO on exercise performance on an individual basis. They were provided information on the effects, dosage, and safety of OxyRBX as well as the benefits on performance. OxyRBX was described as a legal r-HuEPO-like substance shown in animal studies to induce benefits similar to r-HuEPO and was safe for use in humans.
Athletes performed a 3-km familiarization time trial which was used to handicap the 3-km competition runs in the main study. Handicapping means if an individual ran 5 seconds faster than another on their time trial, the slower individual would get a 5 second head start in the actual race. Then participants followed a randomized crossover design with testing before and after a 7 day “control” phase and before and after a 7 day “placebo” phase with 14 days in between. The 14 day gap was sold as a “wash out” phase for individuals who received the OxyRBX. Eight participants underwent the control phase first with the other seven undergoing placebo first.
The primary outcome was participant’s 3-km race time with quantitative variables of mean heart rate, rate of perceived exertion [RPE], hemoglobin (g/dL), hematocrit % (HCT), red blood cell count (x109/L), mean cell volume (fL), and mean corpuscular volume (pg). RPE in this instance was based on the Borg scale from 6 to 20 where 6 = no effort and 20 = maximum effort. Participants were also queried when attending their sessions for daily placebo injections on whether they noticed any changes while taking OxyRBX. Specifically, they were asked if they felt different while “taking” the substance; how they felt during training and races; whether they felt that their recovery was different, and whether they noticed any side effects.
There was also a qualitative arm to the study after the race with research team members asking participants questions pertaining to their experience taking OxyRBX during the trial, whether they thought it would improve their performance, whether they felt different “taking” the substance, how they felt during training and races, whether they felt their recovery was different, and whether they experienced any positive or negative side effects. After individuals had seen their race times they were also asked the extent to which the substance allowed them to work harder. All subjects were debriefed to the nature of the study after completion of the post-race interview.
Study Results
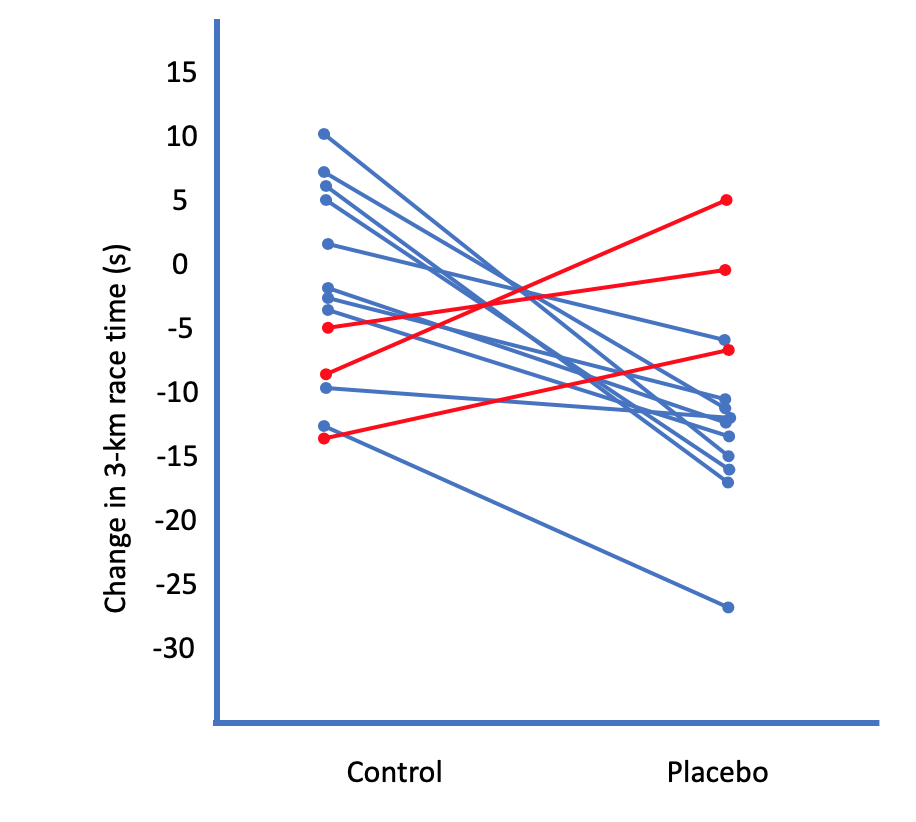
When believing they had taken the placebo drug, individuals demonstrated significantly improved performance in their 3-km races than when exposed to control (9.73 s faster, 95% Confidence Interval (CI), 5.14-14.33 s faster vs. 1.82 s, 95% CI 2.77 s slower-6.41 s faster). Eleven participants improved more in response to placebo than control, one had no change, and three participants had greater performances in response to control.

Figure 2 demonstrates the difference in individual race times in 3-km times between the control group and placebo.. The placebo group amounts to a 1.2% improvement in time compared to the control group. For perspective, in the 2018 men’s 5-km race the difference between 1st and 8th place was 5.27 seconds.
On an individual participant level, figure 3 demonstrates the changes in time for 13 participants, 10 of whom improved their times with the introduction of placebo. There were, however, 3 individuals whose time increased with the introduction of placebo. Those individuals, in the qualitative aspect of the study expressed statements such as “I felt like my legs were really heavy, felt like it was working against me, particularly the drug week.” While the total cohort did improve, it is important to note that some individuals did not, with some times worsening. This is where the qualitative portion of the study can offer insight as to why these results were present.
Athletes were questioned post-study regarding their beliefs with almost all reporting they believed they were taking a real drug. The magnitude of their expectations demonstrated a loose association with the magnitude of their performance.
An individual who experienced a positive response reported, “I wanted to kind of count down until I was going to take it” while another who did not experience any improvement reported “I didn’t think taking the drug would have any effect at all…” The authors attribute the overall effect to motivational intensity theory, which states that maximal exercise tolerance increases when either perception of effort is reduced or “potential motivation” is increased. Marcora 2010
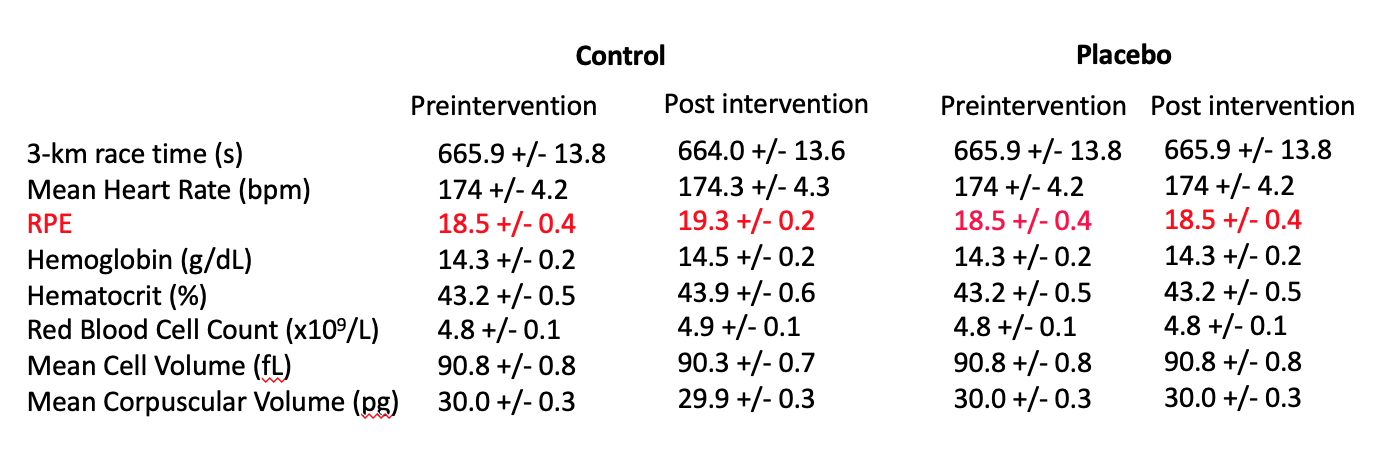
There was no reported difference in hematological variables in either group. Table 1 shows these results. Also, there was no difference in RPE rating between pre and post conditions in either group.
Take-Home Message
There is a lot to unpack with this study, and it was chosen to expand upon those commentaries. First, my selection for the title of this piece “OxyRBC is a proven, safe performance enhancing drug to increase running performance” was intentional. Even though this study was a trial of placebo, and did exhibit positive results, the framing of those results could easily convey the message that this substance caused a real effect on performance. There are numerous supplements on the market that show increased performance attributable to some biochemical change that likely do not fair better than a placebo. Randomized, controlled trials are designed, and often necessary, to pick up any difference between an inert and actual substance. Demonstrating that a substance increases performance in an uncontrolled study does not give good information as to the actual utility of the substance versus the meaning response associated with it.
Unless the reader has seen this study prior, the first inclination upon seeing the title was likely a curiosity to see what this “OxyRBX” is, and what it can offer to athletic performance. The choice of a placebo study on endurance performance for this month’s BMR was also intentional. The large cohort of readers subscribing here have an inclination towards strength sport. It is easier to look at an outgroup and see the flaws in their reasoning. If the reader does not think these same effects are prevalent in strength sports, let me refer them to Ariel et al 1972 and Maganaris et al 2000. Ariel 1972, Maganaris 2000
The first study, from nearly 50 years ago, is a testament to the power of beliefs in training for strength sports. Fifteen athletes with at least two years training experience were instructed they were going to participate in a study on the effects of Dianabol (an anabolic steroid) but only those who demonstrated the best gainzZz in the first 7 weeks of the study would be selected. During those 7 weeks, the selected cohort of 6 individuals for the placebo arm of the study put 11kg on their total for squat, bench press, and seated military press. These six individuals then completed an additional 4 weeks of training while taking a placebo pill that they were informed contained 10mg of Dianabol. I want to reiterate here that these individuals had reported training for at least two years and that they were taking a placebo. How much did their total improve? 45 kilos. This was after 11kg improvement in the prior 7 weeks.
The astute reader will also notice there is a contradiction in key points 2 and 3 at the beginning of this piece. There were no differences in the reported RPE between groups in the pre and post interventions but there was a qualitative reporting of the race feeling easier. Table 1 shows the RPE ratings with the low end being an 18.5 in both groups. A basic conversion to the RPE most readers are familiar with would be approximately RPE 9. This means the athletes were competing near maximum effort which is, in effect, where anyone should be for a competition. Races are judged on the distance they are ran (stating the obvious) and in this case a 3-km. This would be the equivalent of a lifting competition being judged on how fast an individual could squat 405# with time being the variable measured in both. If a competition were to transpire this way, someone with a faster bar speed would likely perceive the task as easier even if they were giving maximum effort.
Overall, this study demonstrates how expectation of benefit can improve performance in some athletes. With the plethora or treatments, ergogenic aids, training templates, recovery tools, passive modalities on the market, the degree to which an athlete believes they work influences if they work. It also raises an ethical dilemma for practitioners and coaches. If research has demonstrated that a performance aid does not work by a physiological mechanism beyond belief, is it okay to use? Also, is it ethical to knowingly misinform athletes that a device or treatment will help them recover faster or perform better using a physiological explanation that is unsubstantiated. The subjects in this study were all debriefed to the fact they were receiving a placebo injection. That does not invalidate the results the athletes achieved regarding their performance. We can continue to apply explanations to treatments such as neurophysiological changes, breaking up adhesions, diffuse noxious inhibitory control, or any other manner of polysyllabic explanation, or we can be honest with athletes that it is ultimately up to them to believe in what they can do and train accordingly. We are also all exposed to the effect our beliefs have on performance. The athletes in this study who believed they would experience a bigger effect did. Those who did not, or experienced anxiety regarding adverse effects of the drug did not.
References
- Ross R, Gray C, Gill J. Effects of an Injected Placebo on Endurance Running Performance. Med Sci Sports Exerc. 2015 Aug;47(8):1672-81.
- Geers A, Miller F. Understanding and translating the knowledge about placebo effects: the contribution of psychology. Curr Opin Psychiatry. 2014 Sep;27(5):326-31.
- Rossetini G, Carlino E, Testa M. Clinical relevance of contextual factors as triggers of placebo and nocebo effects in musculoskeletal pain. BMC Musculoskelet Disord. 2018 Jan 22;19(1):27.
- Beedie C, Foad A. The placebo effect in sports performance: a brief review. Sports Med. 2009;39(4):313-29.
- Beedie C, Stuart E, Coleman D, Foad A. Placebo effects of caffeine on cycling performance. Med Sci Sports Exerc. 2006 Dec;38(12):2159-64.
- McClung M, Collins D. “Because I know it will!”: placebo effects of an ergogenic aid on athletic performance. J Sport Exerc Psychol. 2007 Jun;29(3):382-94.
- Zhang W, Robertson J, Jones A, et al. The placebo effect and its determinants in osteoarthritis: meta-analysis of randomised controlled trials. Ann Rheum Dis. 2008 Dec;67(12):1716-23.
- Nahin R, Barnes P, Stussman B. Expenditures on Complementary Health Approaches: United States, 2012. Natl Health Stat Report. 2016 Jun 22;(95):1-11.
- Carpenter P. Performance-enhancing drugs in sport. Endocrinol Metab Clin North Am. 2007 Jun;36(2):481-95.
- Strano Rossi S, Botre F. Prevalence of illicit drug use among the Italian athlete population with special attention on drugs of abuse: a 10-year review. J Sports Sci. 2011 Mar;29(5):471-6.
- Durussel J, Daskalaki E, Anderson M. Haemoglobin mass and running time trial performance after recombinant human erythropoietin administration in trained men. PLoS One. 2013;8(2):e56151.
- Heuberger JA, Cohen Tervaert JM, Schepers FM, et al. Erythropoietin doping in cycling: lack of evidence for efficacy and a negative risk-benefit. Br J Clin Pharmacol. 2013 Jun;75(6):1406-21.
- Tversky A, Kahneman D. Judgment under Uncertainty: Heuristics and Biases. Science, New Series, Vol. 185, No. 4157. (Sep. 27, 1974), pp. 1124-1131.
- Marcora SM, Staiano W. The limit to exercise tolerance in humans: mind over muscle? Eur J Appl Physiol. 2010 Jul;109(4):763-70.
- Ariel G. Saville W. Anabolic steroids: the physiological effects of placebos. Medicine and Science in Sports. 4(2):124–126, JUL 1972.
- Maganaris C, Collins D, Sharp M. Expectancy Effects and Strength Training: Do Steroids Make a Difference? The Sports Psych. 2000 Sept; 3(14): 272-278. Am J Sports Med. 2007 Mar;35(3):374-83.