
The role of gender in sports dates to the 1890’s and the birth of the modern Olympic movement. When asked about the inclusion of women in the Olympics, the founder of the International Olympic Committee (IOC) and father of the modern Olympic Games, Pierre de Coubertin, said, “Women have but one task: that of crowning the winner with garlands.”Warner 2006 The Olympics of 1900 held in Paris, France allowed women to participate for the first time in just two sports: tennis and golf. Unsurprisingly, women’s participation in the Summer Olympics was low, at about 2% of all participants until 1924, the final year Coubertin was president of the IOC.IOC Factsheet
Over the years, the IOC gradually made strides towards including more competitive opportunities for women as well as leadership roles in sports administration. This has been a slow process, as women were only recently allowed to participate in Olympic Weightlifting at the 2000 Olympic games in Sydney, Australia.IOC Factsheet Additionally, a 2013 survey of over 1,500 individuals holding leadership positions in international sports organizations revealed that only 13% were women, and 14 of the 56 executive committees included no women at all.SportAccord Factsheet Despite this, women’s participation in sport has been rising, as demonstrated by increased presence at the highest level of competition. At the 2012 London Games and 2016 Rio Games, women made up about 44% and 45% of all athletes, respectively. IOC Factsheet
As women’s participation rates have increased, sporting organizations have had to face a new policy question: How do we determine who is eligible for the women’s division? In other words, how do we define “woman” and “man” for the purposes of athletic competition? It is tempting to rely on science — the systematic pursuit of knowledge — to produce policy change, but what if science doesn’t have an answer?
Editor’s note: This article is over 30 pages long with 14,000+ words. We encourage you to read it, however we know many will be looking for a brief summary. There are two sections at the end of the article titled “Recommendations and Conclusions” and “Executive Summary”. Give those a read if you want a condensed version.
The Confused Biology of Sex
Sex and gender, while frequently used as synonyms, are not the same thing. We will not treat them as the same thing here. The notion that sex is a biological designation while gender is a societal construct is often put forth. However, that dichotomy does not hold up to scrutiny, as we will discuss. Some definitions are in order.
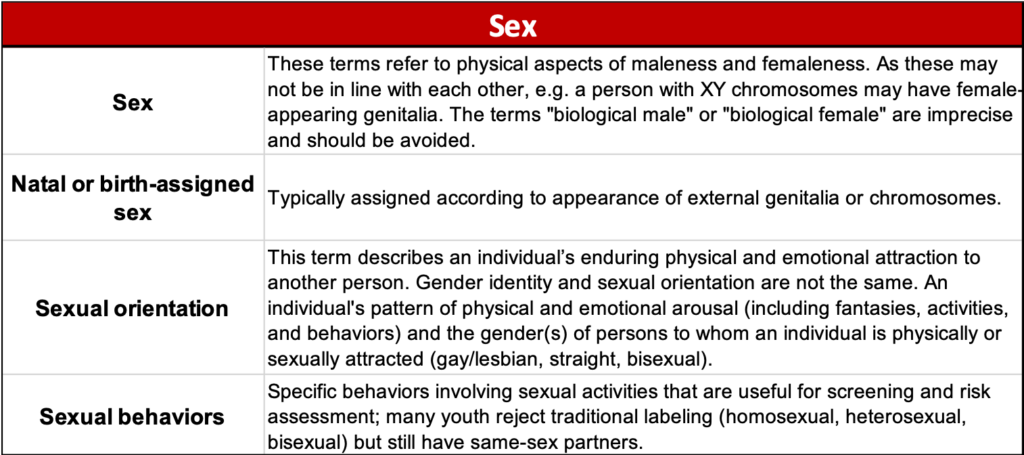
Sex is typically assigned at birth according to the appearance of the external genitalia along with chromosomal composition of the individual (see Figure 1). Perrin 2002 Raveenthiran 2017 Frankowski 2004 The two sexes we are most familiar with are male and female. The distinctions between them are based upon assumed reproductive function regardless of whether a given individual is capable of reproduction. Without putting too fine a point on things, males have a penis and testicles and females have a vagina and uterus, among other structural and chemical differences. The chromosomal arrangement is discussed at greater length below. This is an oversimplification and exceptions abound, but it represents a starting point and explains the basis for the idea that sex is rooted in a binary, biological classification.
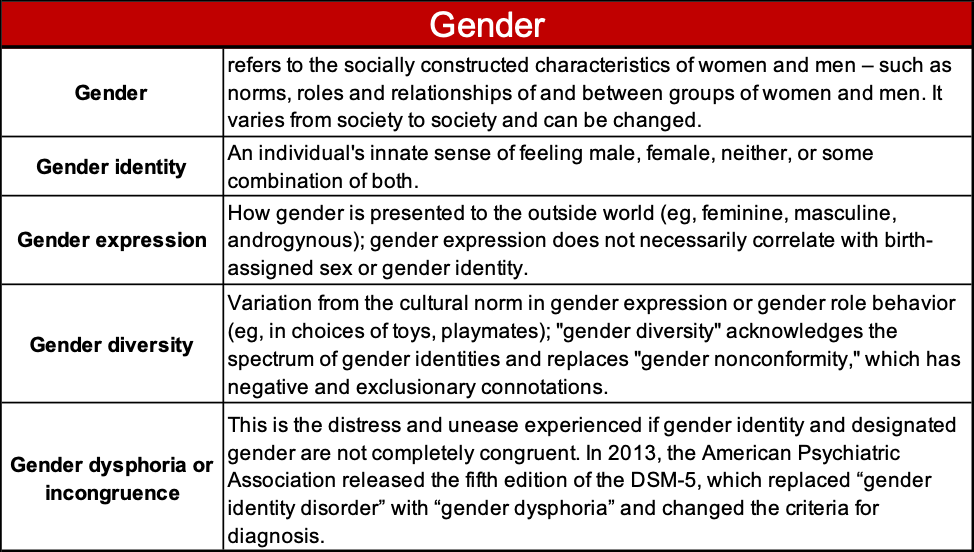
Gender refers to the socially constructed characteristics of women and men, such as the accepted norms, roles, and relationships of and between these groups. Short 2013 While many individuals identify with a gender that aligns with their assigned sex, others do not. Gender resists easy binary classification and exists across a spectrum. There are no externally visible structures that reliably and repeatably predict a person’s gender, nor how they express it. Gender also varies across cultures and its expression can change over time (see Figure 2). WHO Gender and Genetics Adelson 2012
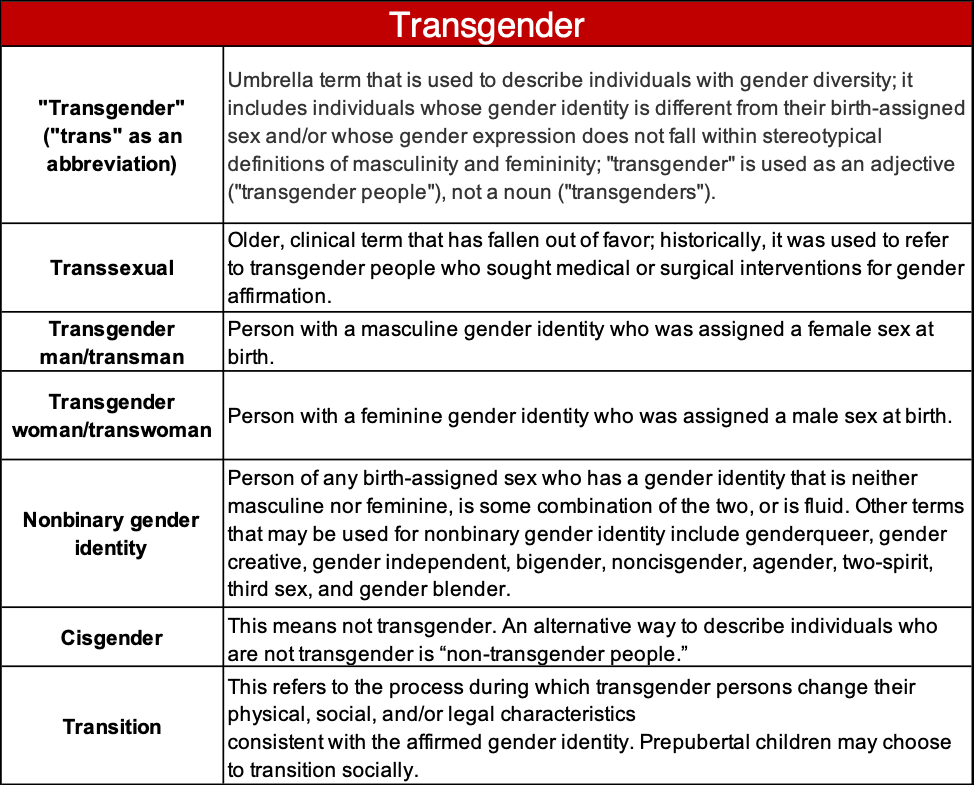
Transgender individuals are people who vary from the cultural norms of gender expression or behavior. This includes individuals whose gender identity is different from their birth-assigned sex as well as those whose gender expression does not fall within stereotypical definitions of masculinity and femininity (see Figure 3). Edwards-Leeper 2012 Rafferty 2018 Hembree 2017 The word transgender is even more loosely defined than sex or gender in part because of its relative novelty from a cultural standpoint. Of particular interest to this discussion are transgender individuals who have actively transitioned from one gender to another with the aid of modern medicine, specifically men who transitioned to women. Transgender men, or transmen, are individuals who transitioned from female to male (FTM). Transgender women, or transwomen, are those who transitioned from male to female (MTF).
Sex and Chromosomes
Humans are typically born with 46 chromosomes, which are DNA (Deoxyribonucleic Acid) molecules carrying genetic information known as their “genotype”. The expression of this genetic coding leads to the physical appearance and manifestations of a person known as their “phenotype”. Individuals inherit 23 chromosomes from each parent during the fertilization process. The first 22 pairs of chromosomes are numbered 1-22, ranked from largest to smallest. The 23rd pair of chromosomes, termed “sex chromosomes”, consist of the “X” and Y” chromosomes. They are also are named according to size with the larger chromosome referred to as X and the smaller chromosome called Y.Keierleber 2019
Most females are genotypically 46 XX, meaning they have 46 chromosomes, including two X chromosomes. Most males are genotypically 46 XY. However, some individuals will be born with just a single sex chromosome (45 X or 45 Y) in conditions known as sex monosomies. Others are born with multiple sex chromosomes (47 XXX or 47 XYY to name a few) in conditions known as sex polysomies. Additionally, some phenotypic males, individuals who “appear” to be male, are born with 46 XX – a more typical female genotype. This can happen when the small Sex-determining Region of the Y chromosome (SRY) is included with the 46 XX chromosome complement.WHO Gender and Genetics Similarly, some phenotypic females are born with 46 XY, the typical male genotype, due to mutations in the Y chromosome that compromise its function.
These examples should help to illustrate that the idea of sex as a genetically binary construction is not supported by the facts. Individuals who do not neatly fit into the “46 XX female” and “46 XY male” paradigm are often described as having a Disorder (or Difference) of Sexual Development (DSD). Lee 2006 Individuals with DSD encompassing the variations described above, as well as others, are seen in approximately 1 per every 1000 to 2000 live births. Blackless 2000 Dreger 1998 Said differently, the prevalence of individuals who are “not XX and not XY” is about 1 in 1666 live births. Dreger 1998
In contrast, the prevalence of 46 XY in the female athletic population is about 7 per 1000 adults, which is 140 times greater than what is seen in the general population. Bermon 2014 For context, of the 4,676 women competing at the 2012 Summer Olympic Games in London, we would predict ~32 women competitors would have a 46 XY genotype.
Gender, Its Distinctions, and Biology
Gender identity and expression are non-binary. Individuals can have an innate sense of feeling male, female, neither, or some combination of both and express it in a variety of ways which can dynamically change based on different social and cultural settings. Still, it would be incorrect to suggest that gender expression and gender identity are self-determined or volitionally chosen by the individual, as there are multiple lines of evidence suggesting it also has a biological basis.
For example, a recent systematic review looked at studies involving individuals with disorders (or differences) of sex development (DSD), which refers to anomalies of the sex chromosomes, the gonads, the reproductive ducts, and the genitalia. Two important studies looked at individuals who were 46 XY and had severe abnormalities, e.g. failure of the penis to form, but no hormonal abnormalities
For many years, the standard treatment for these patients included female gender assignment and surgical feminization, yet some would forgo these treatments and instead be raised as males. While none of the patients raised as males initiated a gender change to female, two studies reported that 22% and 50% of those raised as females later changed their gender identity to male. The authors conclude, “Although the cohort sizes in these studies were small, the data provide the strongest evidence for the biological underpinnings of gender identity.”Saraswat 2015
Twin studies can be useful at determining the genetic and environmental influences of a particular trait or phenotype. Identical twins have identical genetic information, as they result from a single fertilized egg being split into two. Conversely, fraternal twins have different genetic information, as they result from the simultaneous fertilization of two different eggs by two different sperm. By comparing identical twins raised in a shared environment to fraternal twins raised in a separate, shared environment, researchers can gain insight into the genetic underpinnings of a particular phenotype. In the case of the transgender phenotype, when one of the twins identifies as transgender, there is a 40% chance that the other twin will also identify as transgender. Among fraternal twins, there is a 0% correlation in similar circumstances. Heylens 2012 This suggests a genetic influence for transgender individuals.
Additionally, neuroimaging studies show different brain structures and neurophysiology among those with “gender-incongruence”, i.e. those who have a gender identity that is different from their sex chromosomes.Luders 2012 For example, certain areas of the cerebral cortex in both hemispheres are significantly thicker in transgender women than in cisgender men (see Figure 3 for definitions).
Finally, prenatal androgen exposure has been shown to play a role in gender identity formation. Wilson 1999 For example, if an individual with a 46 XY genotype does not receive enough testosterone exposure during gestation – perhaps due to abnormal development of the testes, a defect in one of the enzymes require to make testosterone, or a non-functioning androgen receptor – then the individual can have a phenotype consistent with that of a male, female, and everything in between.
It should be noted that transgender and DSD are not synonyms and we should be careful not to confuse individuals with DSD and transgender individuals, as they are distinctly different. In general, transgender individuals typically do not have a DSD, but identify as gender different than their birth-assigned sex. In contrast, individuals with DSD typically have an anatomical variation, e.g. a individual with a 46 XX genotype who has developed phenotypically male genitalia.
In summary, though there is still much to learn about gender identity and expression, the current evidence suggests that biological factors, in addition to environmental factors, contribute to gender development.
Transgender Individuals in Society and Sport
As of 2016, it is estimated that there are about 25 million transgender individuals worldwide representing 0.3-0.6% of the world’s population. Winter 2016 Despite this prevalence, many transgender individuals experience prejudice, discrimination, and violence due to their gender identity. Claes 2015
For example, a 2018 study of over 120,000 adolescents study found that 50.8% of female to male transgender adolescents had previously tried to commit suicide. Male to female transgender adolescents did not fare much better and reported a 29.9% previous suicide attempt rate. The attempted suicide rates for non-transgender adolescents was 17.6% (female) and 9.9% (male) Toomey 2018 .
As a result, transgender individuals tend to avoid situations where negative interactions (or danger) may occur. In a recent study from the UK, transgender individuals reported specifically identifying avoiding gyms due to fear of harassment from being identified as transgender. Sonja 2014 This is a problem given that physical inactivity is a major contributor to health problems worldwide and is the #4 global risk factor for mortality according to the WHO behind high blood pressure, tobacco use, and elevated blood sugar. WHO 2009. Additionally, transgender people have high rates of depression and anxiety, both of which can be improved with regular exercise and sport. Hep 2005 2018 Physical Activity Guidelines Advisory Committee Scientific Report
At present, the participation rates for transgender athletes in sport are unknown. However, the Olympic Charter – the constitution of the International Olympic Committee- provides support for inclusion of transgender athletes in its Fundamental Principles of Olympism:
Fundamental Principle Number Four
“The practice of sport is a human right. Every individual must have the possibility of practising sport, without discrimination of any kind and in the Olympic spirit, which requires mutual understanding with a spirit of friendship, solidarity and fair play.”
Fundamental Principle Number Six
“The enjoyment of the rights and freedoms set forth in this Olympic Charter shall be secured without discrimination of any kind, such as race, colour, sex, sexual orientation, language, religion, political or other opinion, national or social origin, property, birth or other status.” Olympic Charter 2018
Despite these recommendations, many sporting organizations are having a difficult time squaring the ideals put forth in the Olympic Charter with their current eligibility policies for women and transgender athletes. Deciding which athletes are eligible for the men’s and women’s divisions is complicated by the fact that we cannot identify any single characteristic, or combination of characteristics, that can consistently identify all humans as male or female. Genital structures and chromosomal arrangement all have exceptions and non-binary variations that render them insufficient for the task.
Nevertheless, lines in the sand must somehow be drawn for sports that have gender divisions. History highlights how difficult a task this is when relying only on science.
Gender Eligibility Testing: A Brief History
Prior to 1966 the reports and data on early gender eligibility testing are murky, however it appears that for registration at international events, e.g. the World Championships or Olympic Games, national federations relied on a medical certificate attached to the application form to validate the gender of a female athlete. In many cases, suspicions were raised as to the legitimacy of these documents and subsequently physical examinations were performed on women athletes. Ferguson 1991
Between 1966 and 1967, universal testing of all women was introduced at the 1966 European Athletics Championships in Budapest. According to multiple sources, female athletes were required to walk naked and undergo visual genital inspection by a panel of doctors to obtain eligibility to participate in competitive sport, which were termed “naked parades.” Ferguson 1991, Heggie 2010
Between 1967 and 1996 the IOC used the “buccal smear” test, which is comprised of a swab taken from inside the cheek for DNA testing that allowed doctors to identify the presence of multiple X chromosomes and thus, in theory, provide an objective basis for distinguishing between women and men. The test was found to be unreliable, as it falsely identified women with various genetic make-ups as men. Genel 2005
In 1996, the IAAF and IOC decided to use a different genetic test that identified the sex-determining region of the Y chromosome to again, try to objectively distinguish female from male. The new tests were used in the 1996 Summer Olympics in Atlanta, Georgia where 8 of 3,387 female athletes failed them, although all were allowed to compete as women. Heggie 2010
Starting at the 2000 Summer Olympic Games in Sydney, Australia, the IOC decided to abandon universal testing for female athletes in favor of a “suspicion-based” approach, where athletes suspected of being men competing in the women’s divisions would be tested. This move resulted in no screenings being performed at the Winter Olympic Games of Salt Lake City in 2002, the Summer Olympic Games in Athens 2004, or the Winter Olympic Games in Torino 2006. The suspicion approach ultimately led to officials subjecting athletes like India’s Dutee Chand and South Africa’s Caster Semenya to testing and public scrutiny. We’ll cover this in some detail below.
In 2011 the IAAF published its Hyperandrogenism Eligibility Regulations to help determine, once and for all, who was eligible for the female division in track and field sports. To be eligible, individuals had to be recognized by law as female or intersex, which is a historical term that has been replaced by disorders of sexual development (DSD). Additionally, these individuals must have testosterone levels less than 10 nmol/L for 6 months, which must be maintained during periods where individuals wished to remain eligible. In cases where there was still uncertainty, the IAAF recommended a physical examination to look for “feminine” characteristics, such as lack of body hair, shape of breasts, and the presence of typical genital hair. To accomplish this, the IAAF used The Tanner-Whitehouse Scale.
In April of 2018 the IAAF updated the Hyperandrogenism Eligibility Regulations concerning eligibility for the women’s divisions in track and field sports. Briefly, individuals must be recognized by law as female or intersex, have a testosterone level of less than 5 nmol/L for 6 months prior to eligibility, and maintain this level for the duration of their eligibility period. Of note: all physical exam criteria were removed from the 2018 regulations.
Gender Eligibility Policy is Nuanced
As we can see, determining what gender division an individual is eligible to participate in is complicated. So complicated in fact, that most sporting organizations don’t even try. For example, the International Weightlifting Federation’s (IWF) technical rules for 2019 do not specify any eligibility requirements for participating in a women’s division despite using the word “women” 42 times and “gender” 23 times. They use the word “sex” precisely zero times, though they do have a rule governing the color of the socks or stockings worn by women serving as technical officials. IWF 2019
It appears there is a concern for “gender fraud”, referring to the fear that men will attempt to impersonate women athletes in pursuit of athletic success and accompanying accolades. However, there are precisely zero examples of a man posing as a woman in elite athletics in at least the past 50 years.Pielke 2016
Conversely, there are several examples of women posing as men in order to participate in sport, e.g. Kathrine Switzer using only her initials to run the 1967 Boston Marathon that was closed to women at the time.Switzer 2007 It would seem that gender fraud in sport is an example of an “academic urban legend” – a falsehood repeated so often by academics and others that it comes to be accepted as true.Rekdal 2014
If gender fraud isn’t really “a thing”, then what’s with all the regulation? It would seem as though ensuring a level playing field while fostering participation in sport are the major goals. However, these policies arguably limit eligibility for participation under the guise of fairness. That is, inclusion seems to be permitted only in the demonstrated absence of advantage. Yet some may interpret these policies as discriminatory at worst, or potentially prohibitive when considering cases at the edge of socially-accepted gender norms like Dutee Chand and transgender athletes.
Dutee Chand
Indian sprinter Dutee Chand won two gold medals at the 2014 Asian Junior Athletics Championships in the 100m sprint and 4x400m relays. Due to her impressive performance and “masculine build”, Chand had her testosterone levels tested by the Sports Authority of India.Mohanty 2014 She was found to have a testosterone level in excess of what was allowed by the 2011 IAAF Hyperandrogenism Eligibility Regulations, resulting in a failed test and ineligibility for competition.
Chand appealed to the Court of Arbitration for Sport (CAS), the Swiss-based organization that settles disputes within international sports recognized by the IOC. In July of 2015 the CAS ruled in her favor, stating:
“According to the evidence reported by the IAAF, the competitive advantage that men have over women is approximately in the range of 10 to 12% while that the one enjoyed by hyperandrogenic athletes over other women would be between 1 and 3%. This advantage is not sufficient to justify a separation in the category of female athletes since many other factors such as nutrition, coaching, other genetic and biological variations have an impact on athletic performance.” CAS 2015
Chand was ultimately reinstated and ended up qualifying for the 2016 Summer Olympic Games in Rio in the 100m sprint event, although she ultimately did not advance past the qualifying heats despite her testosterone levels. While the CAS found that Chand may have possessed a 1-3% performance advantage due to her testosterone levels, other factors, such as nutrition, coaching, genetics, etc. also had the potential to similarly impact performance. However, these other advantages and characteristics are not formally regulated in sport, as we’ll see in the case of Eero Antero Mäntyranta.
Eero Antero Mäntyranta
Finland’s distance skier Eero Antero Mäntyranta won five Olympic medals (two gold, one silver, and two bronze) in the 1960s. In endurance events, the oxygen carrying capacity of the blood is an important biological factor in success. Hemoglobin, the protein inside red blood cells that binds oxygen for transport to active tissues, is produced by the bone marrow in response to erythropoietin or EPO, a hormone produced by the kidneys. Athletes use exogenous EPO to increase their hemoglobin levels so that they have more capacity to carry oxygen to active tissues. It is effective in this capacity and is therefore a banned substance in tested sports. With more oxygen carrying capacity, the athletes can work at higher intensities for longer periods of time.Momaya 2015
EPO works by binding to the EPO receptor on cells in the bone marrow. When EPO binds to the receptor, the cell starts making hemoglobin. There is a portion of the EPO receptor that modulates this response, so that the cell doesn’t make too much hemoglobin, as this can cause a variety of health problems. With that in mind, what would happen if an individual had a mutation in the EPO receptor that resulted in a broken “stop” signal, so the cell never gets the message that there was already enough hemoglobin being produced? The individual would have excess hemoglobin production, almost as if they were using exogenous EPO as a performance enhancing drug.
Well, Mäntyranta, and much of his family, happen to carry such a genetic mutation. His EPO receptor gene has a small anomaly that results in a hemoglobin level approximately 65% higher than everyone else not taking EPO.Epstein 2013
Prior to the introduction of the biological passport in 2002 which follows many blood metrics over time to look for signs of doping, the Union Cycliste Internationale (UCI) and Federation Internationale de Ski both placed upper limits on hemoglobin levels to deter individuals from using EPO. However, science showed that hemoglobin levels varied wildly among athletes and did not correlate reliably to performance. A more nuanced approach was needed to determine eligibility for sports participation, e.g. the biological passport in this case.
Interestingly, other genetic conditions have largely been ignored with respect to eligibility. For example, gigantism (e.g. Romania’s basketball player Gheorghe Mureșan) or Marfan’s syndrome (e.g. US volleyball player Flo Hyman) in professional sports. Both conditions result in increased height and limb length, yet we don’t have height or limb length cutoffs in these sports. Nor do we use testosterone levels to determine male eligibility in sport. Rather it is used solely for the purpose of determining eligibility in women’s sport by organizations using the IAAF’s Hyperandrogenism Eligibility Regulations.
Transgender Athlete Eligibility
At present, there are multiple different policies put forth by international organizations. Most of them have similar requirements to the IOC, which is listed in full below:
International Olympic Committee (IOC):
- Those who transition from female to male are eligible to compete in the male category without restriction.
- Those who transition from male to female are eligible to compete in the female category under the following conditions:
- The athlete has declared that her gender identity is female. The declaration cannot be changed, for sporting purposes, for a minimum of four years.
- The athlete must demonstrate that her total testosterone level in serum has been below 10 nmol/L for at least 12 months prior to her first competition (with the requirement for any longer period to be based on a confidential case-by-case evaluation, considering whether or not 12 months is a sufficient length of time to minimize any advantage in women’s competition).
- The athlete’s total testosterone level in serum must remain below 10 nmol/L throughout the period of desired eligibility to compete in the female category. IOC Consensus 2015
The other organizations listed below tend to have similar procedures to the IOC, although there are some notable differences:
- National Collegiate Athletic Association (NCAA): The NCAA differs from the IOC in that it requires Female-to-Male (FTM) trans athletes to obtain a medical exception for treatment with testosterone for diagnosed Gender Identity Disorder or gender dysphoria and/or Transsexualism. These individuals are no longer eligible to compete on a women’s team without changing that team status to a mixed team. While there are no set cut-offs for testosterone levels published for either FTM or Male-to-Female (MTF) trans athletes, MTF athletes must have documentation of testosterone suppression for one year prior to being eligible to compete on a women’s team. That being said, MTF athletes can compete prior to the full one year of suppression, but the women’s team designation will be changed to “mixed team” status until completion of one year of suppression. NCAA Inclusion of Transgender Student-Athletes 2011
- CrossFit: CrossFit follows the IOC’s lead in all policies outside of requiring legal documentation of their gender, such as a state ID or driver’s license. They also include a provision for transgender women athletes that requires total testosterone levels to be kept below the IOC’s cut-off of 10 nmol/L. Of note, they also make a separate provision for women who may have a DSD or other medical condition that results in a total testosterone level of > 10nmol/L. In these cases, these athletes must demonstrate that they have a genetic condition that affects the bioavailability of their serum testosterone, such as hyperandrogenism, androgen insensitivity syndrome, or 5-alpha reductase deficiency. CrossFit Rulebook 2020
- United States Weightlifting (USAW): The USAW uses the IOC’s policy for the most part, though they do require more extensive documentation and hormonal suppression. Athletes wishing to change their gender identity need to have a written letter requesting eligibility to participate as a different gender, a confirmation of gender identity from a medical professional, and legal documentation of their identified gender. With respect to hormonal suppression in MTF athletes, the USAW requires two years of hormone therapy, instead of just one as required by the IOC, to minimize gender related competitive advantages. For FTM athletes desiring hormone therapy, documentation must be provided certifying the athlete’s therapy is being monitored by a medical doctor and is not being used as a way to enhance athletic advantage.USAW Transgender Policy
- United States of America Powerlifting (USAPL) and International Powerlifting Federation (IPF): While both organizations recognize the IOC’s policy on transgender participation in sports, there is only limited opportunity for transgender athletes to participate. Specifically, transgender women are not allowed to compete in the women’s division but are allowed to compete in the men’s division. If they are taking spironolactone, a common anti-androgen used in combination with synthetic estrogen for transitioning individuals, they must obtain a therapeutic use exemption (TUE) in order to participate and comply with existing WADA regulations. Transgender men, or any athlete taking testosterone, may not participate in USAPL or IPF competitions, with or without a Therapeutic Use Exemption form. No TUEs are available in USAPL or IPF for testosterone therapy. However, transgender men may participate in the men’s division if they are not taking testosterone or any other prohibited substances. USAPL Transgender Policy
At present, it appears that registering for an event sanctioned by CrossFit, USAW, or IAAF requires transgender women to maintain testosterone levels of less than 10 nmol/L for a period of either 1 year (CrossFit and IAAF) or 2 years (USAW) to be eligible for the women’s division. Conversely, no objective limits have been placed on transgender men for testosterone levels, despite receiving exogenous testosterone support.
Again, none of the organizations listed here define sex or gender for the purposes of participation eligibility. This bears repeating. Nobody has definitively said who is and who isn’t a female or a male (or man or woman). Further, none of the organizations list testing policies and procedures for sex or gender verification, which follows the IOC’s decision from 2000 to eliminate routine sex testing in individuals.
When discussing this issue with the USAPL’s TUE Chair, Dr. Kris Hunt, he lamented that there isn’t any way to do this objectively and even if there were, the costs would likely be prohibitive. Personal Communication Hunt 2019 For those concerned about equity in sport, we lack any criteria beyond self-reporting to establish gender separation for athletes.
To summarize, sporting organizations do not have technical procedures for identifying who is eligible for the women’s or men’s division outside of the necessary legal documents required to register for competition and the testosterone cut-offs described above. However, transgender athletes appear to have a number of barriers to participating in sport based on the premise of “fairness” in competition. Policy-makers are looking to science to answer the question: Do transgender athletes have a competitive advantage?
The Gender Gap In Performance
One way to attempt to answer this question is to look at the performance gap between cisgender athletes. In doing so, researchers may be able to predict what competitive advantage, if any, persists after an individual transitions.
A 2010 paper by Thibault et al. measured the difference between the top 10 performers’ results from each gender across a wide variety of different events. The authors report:
“A stabilization of the gender gap in world records is observed after 1983, at a mean difference of 10.0% ± 2.94 between men and women for all events. The gender gap ranges from 5.5% (800-m freestyle, swimming) to 18.8% (long jump). The mean gap is 10.7% for running performances, 17.5% for jumps, 8.9% for swimming races, 7.0% for speed skating and 8.7% in cycling. The top ten performers’ analysis reveals a similar gender gap trend with a stabilization in 1982 at 11.7%.”Thibault 2010
The 10-12% difference in performance between different genders has been corroborated in several other reviews, with exceptions in events where upper-body power is a major contributor and in ultra-endurance swimming. In the sports reliant upon upper-body power, the gender gap is larger, at more than 15%. In ultra-endurance swimming the gap is now less than 5%. Sandbakk 2017
However, there’s some nuance here, as different results emerge when we consider individual sports. Consider that the gender gap in Olympic weightlifting is at 36.8%, which is far greater than the average difference of 10-12% cited above.Thibault 2010 An even larger gap is seen when comparing international-level powerlifters. A recent review of competitors in the International Powerlifting Federation (IPF) conducted by their affiliate federation, USA Powerlifting (USAPL), showed approximately a 40-70% difference in strength performance between men and women, depending on what kind of statistical analysis was used.Personal Communication Hunt 2019
One way to look at this is to suggest that some biological factor such as testosterone, presence of a Y-chromosome, growth hormone levels, or some combination of biological factors have a greater opportunity to widen the gap in barbell sports when compared to sports where the focus on absolute strength is not as significant and the gap is lower.
A 2018 review by Handselman et al., suggests the evidence for all these biological factors, save for testosterone, is fairly weak. For example, the presence of a Y chromosome was thought to result in the 10-15 cm height difference between men and women, which subsequently resulted in greater muscle mass given that height is correlated with muscle-mass-carrying-capacity. However, the only gene on the Y chromosome associated with an effect on height is the short stature homeobox (SHOX) gene, which has a dose-dependent effect on height in humans. In other words, the more copies of this gene a person has, the taller they grow. As it turns out, the SHOX gene is located on both the X and Y chromosomes – not just the Y chromosome. Individuals with the genotypes 47 XYY and 47 XXY are approximately the same height, which suggests the Y chromosome’s genetic effect on height is insignificant, if present at all. Handsleman 2018 The effect of different testosterone levels on the performance gap is a different story and will be discussed separately.
On the other hand, one might observe the larger gender gap in barbell sports and wonder whether there may be other, non-biological factors involved. For example, women weren’t allowed to compete in Olympic weightlifting at the Olympics until the 2000 Summer Games in Sydney.Thibault 2010 Additionally, about 50 world records in women’s weightlifting are set by Chinese athletes, which speaks to both the success of the Chinese recruitment and development systems as well as the relative competitiveness compared to the men’s divisions.Guillaume 2009 In the case of powerlifting, a women’s division was added to the Bench Press in the 2000 Paralympic Games in Sydney while men had been competing since 1992. Paralympic 2016 The earliest available data available for women competing at the non-Olympic international level was from the 5th World Games, held in Finland in 1997, The inaugural World Games in 1981 featured only men’s divisions.World Games Results
Competitiveness is driven by several factors, one of which is participation rates. Larger pools of competitors tend to increase the probability that there are multiple standouts, which drives competitiveness (and records) up. Consider the following: it wasn’t until the 2012 Summer Olympic Games in London that every country’s delegation included a female competitor for at least one sport. Capranica 2013 Additionally, the latest data on USAPL’s over 22,000 members indicate a 2:1 ratio of men to women as of 2018 memberships, up from a previous ratio of 4:1 in 2014. Taken together with the short history of women’s participation in barbell sports, psychosocial and cultural factors could be important contributors to the larger gender gap seen in barbell sports.Capranica 2013 In other words, we may not yet know what women can do in this arena because we do not yet have a representative sample.
Based on the present evidence, it is reasonable to suggest that biological, psychological, and sociocultural factors contribute to the range of gender gaps observed across sports. Sports with a long history of women’s inclusion and large athlete pools, such as running, cycling, and swimming demonstrate the 10-12% performance gap, even for sprint events like the 100 m race and all 100 m swim events. Sandbakk 2017
Conversely, sports that require more upper-body muscle strength, e.g. canoeing, kayaking, and skiing, tend to have a gender gap of around 15%.Sandbakk 2017 Finally, the gender gap is actually reversed in open-water ultra-endurance swimming. Women hold the records for both the 32-km ‘Catalina Channel Swim’ and 46-km ‘Manhattan Island Marathon Swim.Knechtle 2014 However, with ultra-endurance swimming, we may also suffer from a smaller than representative sample size. Of the four fastest swims at Catalina, only one was measured within in the last seven years, and one of the records is over four decades old. Despite this, the current data on powerlifting and Olympic weightlifting suggest a nearly 3-fold increase in the performance gap between genders, which may be inflated by non-biological factors such as participation and coaching access, sociocultural factors, and inequality at every level of sport, among others.
Nevertheless, there are certainly real biological differences between men and women that we should address:
Height: On average, men tend to be 10-15 cm taller than women. It is thought that testosterone release during puberty is responsible for the average greater height in men. Courant 2010
Muscle Mass: On average, men tend to carry 30-40% more lean body mass than women (this includes muscle, organ, bone, water, and all other non-fat mass).Janssen 2000 However, height and weight influence muscle carrying capacity for an individual regardless of sex or gender. Heymsfield 2015,Gallagher 1997 Interestingly, when correcting for height and total body weight, the gap narrows to an approximately 10% average difference in lean body mass between men and women across the entire lifespan. Kirchengast 2010 Men and women exhibit a similar relative increase in muscle hypertrophy in response to resistance training as well. Abe 2000
Strength: Muscular strength can be defined as force production measured in a specific context. Based on small data sets, it is reported that men have 48% and 34% greater strength than women in the upper and lower body muscles, respectively. Miller 1993 However, no differences in strength between men and women are seen when normalized for muscle cross-sectional area. Miller 1993 Bishop 1987 Hannah 2012 Additionally, men and women exhibit similar relative responses to resistance training, with no gender-specific responses noted after 10-weeks of resistance training. Gentil 2016
Finally, a number of other gender-independent factors contribute to the regulation of adult muscle mass, including genetics, race, adiposity, training, diet, and birth order. Heymsfield 2015 For example, data from twin studies suggests up to 50% to 60% of the difference in muscle mass and strength may be due to genetic factors without clear gender influences. Silventoinen 2003, Beunen 2004, Silventoinen 2008 Said differently, the amount of muscle mass and strength displayed by an individual may be influenced by non-sex genetics to a level that rivals or exceeds the influence of gender.
Power: Muscular power can be defined as high-velocity force production. As described above, men tend to be taller, heavier, and carry more muscle and less body fat than women. Despite men having more muscle mass however, there does not appear to be any difference in average muscle fiber type composition (e.g. Type I- and Type II fibers) between genders. Miller 1993 Type I muscle fibers are classically referred to as “slow-twitch” muscle fibers and tend to produce low amounts of force for long periods of time, e.g. they are very fatigue resistant. In contrast, Type II muscle fibers, or “fast-twitch” muscle fibers, tend to produce high levels of force for short periods of time and are tend to fatigue quickly.
Interestingly, muscle fiber type composition seems to be more strongly correlated with training history and athlete caliber than gender. Serrano 2019 For example, women who compete in Olympic weightlifting at the World or Olympic level were found to have 71% fast-twitch type IIa fibers compared to the 63% seen in men competing at the National level. Serrano 2019
While absolute power output appears to be greater in men in general, when we normalize existing power data for fat-free mass and fat-free cross-sectional area (approximating the amount of skeletal muscle mass) there are few, if any, gender-specific differences in power. van den Tillaar 2004
For example, Slawinski et al. looked at peak acceleration after 1 second in 100 world-class sprinters (50 women and 50 men). After normalizing for body mass, men and women had approximately the same peak acceleration power. Slawinski 2017 This study is unique given the relatively large sample size of 100 and the findings. Nevertheless, the generalizability of these results be limited given that all subjects were already world-class sprinters and thus, not generalizable to untrained individuals.
Additional evidence from researchers in Spain provides insight here: 155 college-aged, untrained individuals (123 men and 32 women) tested their anaerobic power output using a Wingate cycling test, which showed no differences between men and women when normalized for fat-free mass. Perez-Gomez 2008
Body Fat: As mentioned above, men tend to have 10% greater lean body mass than women of the same height and weight, while women have about 10% greater body fat than men. This gap also tends to be preserved over the entire lifespan. Kirchengast 2010
Hemoglobin: As described above in the Eero Mäntyranta story, hemoglobin is responsible for carrying oxygen around to active tissues. On average, hemoglobin levels are 12% higher in males than females, which is thought to be due to the effect of testosterone.Shahani 2009
Testosterone: In healthy males, total testosterone ranges between 250 – 1000 ng/dL are considered normal, with some slight variation on the upper and lower limits depending on the laboratory and age of the individual.Morales 2015 This wide range does not appear to confer an athletic advantage, however. Individuals with endogenous testosterone levels the higher end of normal do not tend to outperform individuals with testosterone levels at or near the lower end. Karkazis 2012 Morton 2018 Morton 2016
Experimental evidence reflects a nearly 5-fold difference in average testosterone levels between your typical man and woman. Clark 2018 This produces the much lower normal total testosterone range for women of 20-60 ng/dL, with additional variation based on the lab and phase of the menstrual cycle. Clark 2018 Longcope 1986 When it comes to athletes however, things are not so clear. A 2017 study found that 101 of 795 (13%) men had free testosterone levels that were within the reference range for cisgender women without DSD (<0.23 nmol/L). Bermon 2017 Regardless, as seen with men testosterone ranges- free or total- in women do not neatly and reliably correlate to performance.
Returning to the aforementioned Dutee Chand case for a moment, the Court of Arbitration in Sport said, “The Panel has accepted that testosterone is the best indicator of performance difference between male and female athletes. However, the evidence does not equal the level of testosterone in females with a percentage increase in competitive advantage.”CAS 2015 In other words, even though Chand’s testosterone levels exceeded the normal female range, the panel could not find convincing evidence that this conferred an advantage that could be quantified. Indeed, Chand did not even make it into the final heats, let alone medal in the 2016 Games.
In 2012, Dr. Katrina Karkazis and Dr. Rebecca Jordan-Young, two influential bioethicists published a landmark paper titled “Out of Bounds, A Critique of the New Policies on Hyperandrogenism in Elite Female Athletes” in the American Journal of Bioethics. In this article, the authors reviewed the controversies over eligibility policies and conclude with respect to testosterone:
“Despite the many assumptions about the relationship between testosterone and athletic advantage, there is no evidence showing that successful athletes have higher testosterone levels than less successful athletes.” Karkazis 2012
Still, the IAAF continues to use testosterone levels to determine who is eligible for the women’s division. In the recent case between the IAAF South African runner, Caster Semenya, the IAAF has produced data suggesting that women with testosterone levels in the highest tertile (one third) had a competitive advantage compared to women competitors with testosterone levels in the lowest tertile. Specifically, women with the highest free testosterone tertile performed better in the 400m, 400m hurdles, 800m, hammer throw, and pole vault with margins of 2.73%, 2.78%, 1.78%, 4.53%, and 2.94%, respectively. Bermon 2017.
However, there were a number of problems with this analysis including duplication of data that skew the results, use of data that cannot be corroborated by actual event results, and ignoring results showing negative correlations between testosterone levels and performance. There were examples of women with higher testosterone levels that underperformed in strength/power events like the 100m (-2.63%), 100m hurdles (-1.69%), 200m (-1.59%), and javelin (-2.53%) when compared to women with lower levels. Bermon 2018 To summarize, these events showed women with the highest testosterone were at an apparent disadvantage.
Consider that when the data are averaged across all events, the advantage for running events is only 0.31% and 1.07% for non-running events. There is also no consistent correlation between performance level in men and testosterone levels.Bermon 2018 This suggests the purported “advantage” presented by the IAAF is an artifact. Due to these errors in the use and reporting of this data, the British Journal of Sports Medicine has been asked to retract the initial paper. Pielke 2018
Sports are divided into women’s and men’s categories, not “low testosterone” and “high testosterone” divisions, or any other biological variable for that matter. Solely focusing on testosterone may be ill-advised. The CAS added the following in the case of Dutee Chand:
“The Panel found that the Athlete has established that it is prima facie discriminatory to require female athletes to undergo testing for levels of endogenous testosterone when male athletes do not. In addition, it is not in dispute that the Hyperandrogenism Regulations place restrictions on the eligibility of certain female athletes to compete on the basis of a natural physical characteristic (namely the amount of testosterone that their bodies produce naturally) and are therefore prima facie discriminatory on that basis too.” CAS 2015
Overall, the size and sources of the performance gap in sport are complex and not-yet fully characterized. While it appears that there are real differences in biological inputs such as testosterone, muscle mass, height, and hemoglobin levels (among others), it is also clear that gender-independent factors such as genetics and training, in addition to non-biological factors like equality in participation opportunities, play substantial roles in performance. It is also unclear what role this science should play in determining policies for gender eligibility in sport, particularly as it applies to transgender athletes.
Do Transgender Athletes Have an Advantage?
Another way to assess the performance gap, if any, between transgender women and non-transgender women in sport is to look at women with hyperandrogenism. Women with this condition have testosterone levels that approach, and in some cases exceed, the lower end of the normal range for men for much, if not all, of their lives. Hyperandrogenism occurs in 5-10% of women due to DSD, Polycystic Ovarian Syndrome (PCOS), Congenital Adrenal Hyperplasia (CAH), and other medical conditions. Yildiz 2006.
Dutee Chand’s case is again relevant. The CAS weighed in on this issue using a panel of medical experts:
“According to the evidence reported by the IAAF, the competitive advantage that men have over women is approximately in the range of 10 to 12% while that the one enjoyed by hyperandrogenic athletes over other women would be between 1 and 3%. This advantage is not sufficient to justify a separation in the category of female athletes since many other factors such as nutrition, coaching, other genetic and biological variations have an impact on athletic performance.” CAS 2015
This CAS ruling suggests that women (gender), specifically those with a DSD or other medical condition, who are exposed to elevated levels of testosterone for most if, if not all, of their life do not have an “unfair” advantage in sport. This may set a precedent for transgender women interested in athletic participation. A competitive advantage of less than 3% would potentially grant them eligibility to participate in the women’s division. Conversely, a competitive advantage of 10-12% or greater would require a different solution for inclusion into sport if this precedent is followed.
Another way to assess whether transgender athletes have a competitive advantage is to look at published research on transgender individuals. At present, there are only a handful of published studies that report objective data on the effects of gender transition on the musculoskeletal system. The dearth of direct evidence on this topic may have implications on the role science should play in policy-making.
Gooren et al.
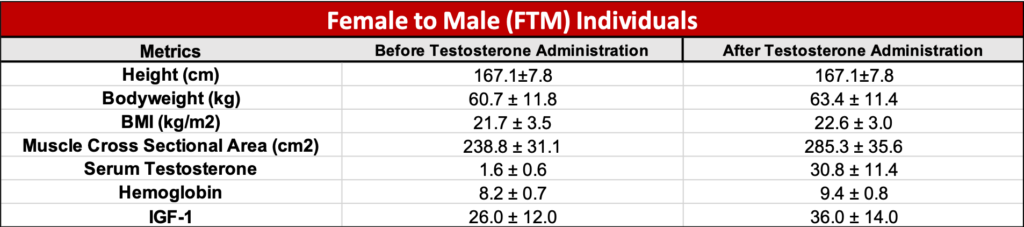
The first paper is from leading experts in endocrinology and transgender medicine, Drs. Louis Gooren and Mathijs Bunck, and was published in 2004 in the European Journal of Endocrinology. The detailed measurements and relatively large sample size make it particularly interesting., Pre-transition data for participants can be seen in Figure 4.

With respect to the transitioning process, the FTM individuals received 250 mg of testosterone every two weeks via injection, whereas the MTF individuals underwent hormonal suppression using an anti-androgenic compound, which was stopped after the first 2 years, followed by indefinite treatment with the synthetic estrogen. Data was collected prior to transition and after 1 and 3 years.
A brief aside, cyproterone acetate is a medication brought to market as an oral contraceptive for women (in combination with estrogen) in Europe in the 1970’s and later Canada in the 1980s. It was never approved for use in the United States. With respect to its anti-androgenic effects, its anti-androgenic mechanism of action is interesting, as it involves inhibition of s Luteinizing Hormone (LH) release from the pituitary gland. In response to this reduction in pituitary LH secretion, the testes produce less testosterone. Cyproterone also blocks the binding of dihydrotestosterone (DHT), which is a potent metabolite of testosterone that has a greater affinity for the androgen receptor when compared to that of testosterone. .Neumann 1999
In the United States, spironolactone (trade name Aldactone) is the most widely used drug for transgender women (ei.ge. MTF individuals). Mechanistically, spironolactone inhibits binding of testosterone to the androgen receptor (ei.ge. competitive inhibition) and prevents the testes from making testosterone.
Spironolactone can be prescribed off off-label to treat hormonal acne (ei.ge. acne vulgaris) in adult women. Zaenglein 2016 Additionally, spironolactone is commonly prescribed as an adjunctive treatment for hirsutism (facial hair growth) associated with polycystic ovarian syndrome (PCOS) if initial treatment with oral contraceptives produce suboptimal results.Martin 2018 With that being said, spironolactone is currently on the World Anti-Doping Agency’s prohibited substance list, as it can be used as both a masking agent and a diuretic.WADA 2019 However, athletes can have their physician submit a request for a therapeutic use exemption or “TUE” in order to use spironolactone outside of competition, e.g., although the athletes must stop using the medication 5 days prior to competition.
Interestingly, the USAPL has performed a retrospective internal data review on female powerlifters who received a TUE for spironolactone to characterize the effect of the medication on strength performance. Based on the data of from ~25 female competitors, it appears that there is a reduction in short-term strength performance (e.g. powerlifting total) in the short- term, which can be negated via continued long-term training. Personal Communication Hunt 2019
Back to the Gooren et al study, which found that body weight increased by 3.4 kg (7.5 lb) while muscle cross-sectional area increased by nearly 47 cm2 in FTM individuals after one year of testosterone administration (see Figure 5). Data from these same authors show a slight reduction in thigh muscle cross sectional area to 280 cm2 after three years of hormone suppression, suggesting a likely plateau in muscle mass accrual when bringing testosterone levels up to that of a “eugonadal” male.
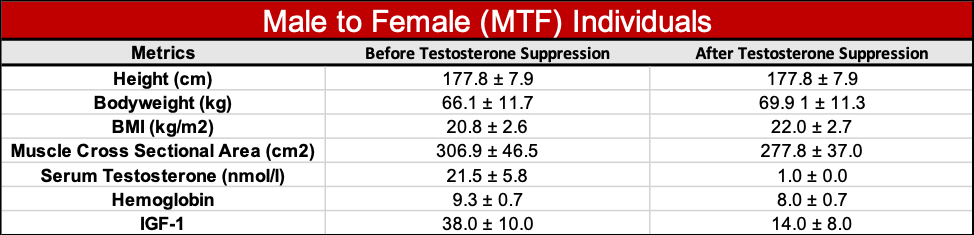
In MTF individuals undergoing hormonal suppression, Gooren et al. found that body weight increased by 3.8 kg (8.3 lb) while muscle cross-sectional area dropped by nearly 40 cm2 after 1 year, which represents an increase in body fat and loss of muscle mass (See Figure 6). Hemoglobin and IGF-1 also decreased, which likely corresponds to the reduction of testosterone to castration levels. Finally, data from these same authors show a further reduction in muscle cross sectional area to 271 cm2 after three years of hormone suppression.
Quantitative comparisons for muscle cross sectional area at the thigh were also made between the subjects prior to transitioning and after hormonal suppression or administration had taken place for one year, as shown in Figure 7.
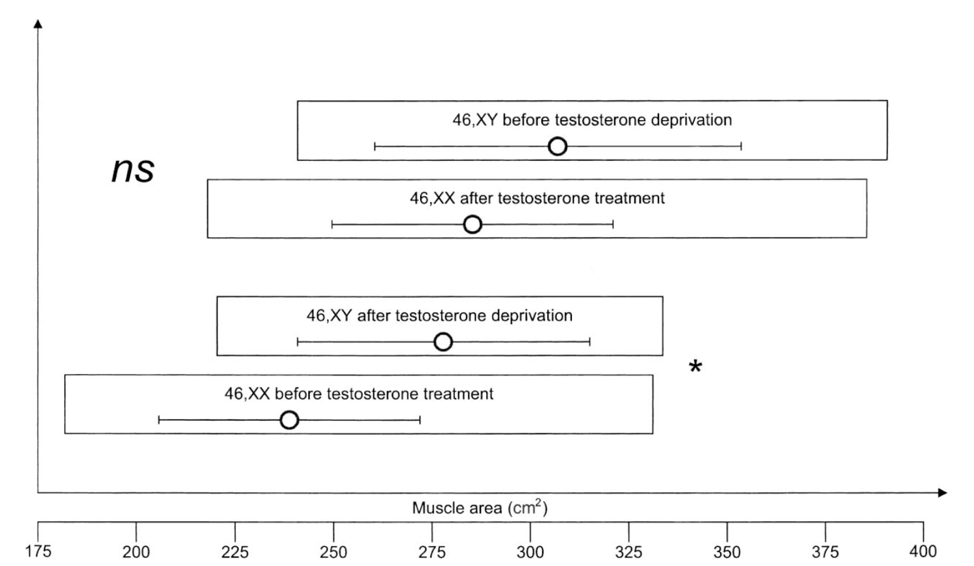
Notice the significant overlap in muscle cross sectional areas between all of the subjects. The mean cross-sectional areas, labeled with an empty circle, suggest that pre-transition men (46, XY) tend to have greater muscle cross sectional area than pre-transition women (46, XX). However, we can also see the considerable overlap between transgender women (46, XY after testosterone deprivation) and cisgender women (46 XX before testosterone treatment).
While the average amount of muscle cross-sectional area in transgender women is about 39 cm2 higher than cisgender women, the overlap in range of muscle cross sectional areas is remarkable. The authors observed this as well, remarking:
“After 1 year of androgen deprivation, mean muscle area in MTF had decreased significantly but remained significantly greater than in FTM before testosterone treatment, though with an overlap that was almost complete when androgen-deprived MTF were again compared to untreated FTM.”Gooren 2004
Harper et al. and T’Sjonen et al.
Two other papers attempt to further characterize musculoskeletal and performance changes in transgender individuals. First up, the 2015 paper by Dr. Joanna Harper, Race Times for Transgender Athletes.
For some background, Joanna Harper is a medical physicist, distance runner, and advisor to the IOC on matters of gender and sport. She was instrumental in developing the 2015 IOC transgender policy and advises on matters of gender and sport. She is also a transgender woman. In her 2015 study, she compared race times of 8 transgender women before and after transitioning. She reported:
“Collectively, the eight runners were much slower in the female gender; slow enough, in fact, that their age-graded performances were almost identical to their male AGs [age gradings*-see below]. Two of the runners had higher average AGs in male gender than in female gender, while one runner had higher female AGs than male ones. The changes in the age grades of these runners mirrored changes in their training habits.”Harper 2015
*AG= age grading, a method of comparing the performance of athletes for all ages and both sexes. For running events, the athlete’s race time (RT) is compared to the fastest time ever run by a person of that age and sex, or the age standard (AS)
The sample size here is small, so the results must be viewed in that light. However, at least in the cases of these eight individuals, transitioning to female resulted in race performances that mirrored their gender-adjusted gradings. They did not become better runners as women than they were as men.
The third study by T’Sjoen et al. looked at 50 individuals who transitioned from male to female with anti-androgen medication and sex reassignment surgery. After 12 months of hormone replacement therapy (HRT), they reported “strikingly lower muscle mass” and increased fat mass compared to pretreatment values and reference controls. However, no absolute values for change in muscle or fat mass were reported.T’Sjoen 2009
Wiik et al.
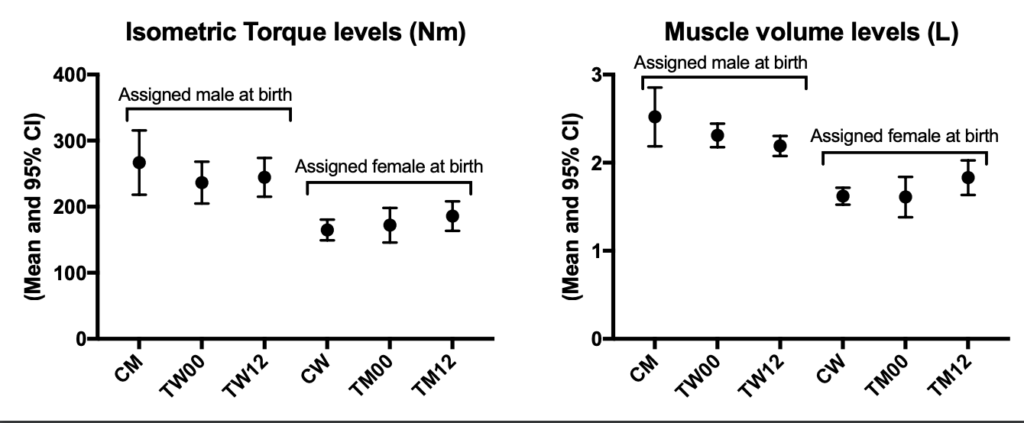
A new paper by Wiik et al takes a look at strength and muscle mass levels in 11 MTF (trans women) and 12 FTM (trans men) individuals over 1 year of transitioning. Strength was assessed using a specialized seated leg machine that constrains the movement velocity and range of motion in order to generate uniform results. In short, the subjects were told to produce as much force as possible for 5 seconds using either leg extension or flexion. Knee extension and flexion values were measured at baseline, 1 month, 3 months, and 12 months. Additionally, muscle cross sectional area and volume were assessed by CT and MRI, respectively, at the same time points.
Similar to the Gooren et al paper, the results of the study show that the trans women individuals lost muscle mass (-5% total thigh volume) whereas trans men individuals gained muscle mass (+15%). At 12 months, the trans women continued to have greater apparent muscle mass than trans men.
With respect to strength, trans men showed an average improvement in isometric knee extension (10%) and flexion (26%) whereas the trans women’s strength did not change. While knee extension strength tended to be higher in trans women throughout the study, knee flexion strength did not differ in trans men compared to trans women.
As seen in Figure 8, the authors compared the transgender individuals’ muscle torque and muscle volume to cisgender controls. However, it is not clear if these controls had similar activity levels, dietary intakes, and/or completed the same strength testing protocols as the transgender subjects. For example, it is well known that repeated exposure to a particular exercise test tends to result in an improved performance in that test. This is evident in this paper in fact, as both trans women and trans men improved their isometric and isokinetic strength throughout the study with repeated testing. Therefore, it is possible a higher discrepancy in these strength measures would be seen between cis men and post-transition trans women would be seen if the cis men also repeated the strength tests 4 times.
Another issue with this study is that none of the individual’s outcome data are reported, i.e. we do not know how much strength or muscle mass was gained (or lost) for each individual. This is problematic for interpretation, as we know that there are large variations in rates of adaptation to exercise (or lack thereof) in humans. Thus, we’d predict some trans women would lose a lot of strength and muscle whereas others would lose less (or potentially gain). Conversely, we’d expect that some trans men would gain a lot of strength and muscle, while others would gain less (or potentially lose).
Taken together with the Gooren et al. and T’Sjoen et al. studies discussed above, muscle mass decreases markedly after transition among MTF individuals. However, despite the overlap in muscle cross-sectional area between cisgender women (pre-transition) and transgender women, it appears that transgender women may carry more muscle mass than cisgender women at 1-year post-transition on average. Additionally, as of this publishing, none of the available peer-reviewed literature has directly measured other objective performance outcomes in sport (e.g. strength, power, VO2max, etc.) outside of Harper’s report on race times pre- and post-transition.
Two additional reviews have recently been published by Hilton et al. and Harper et al. provide additional support that MTF individuals have greater muscle mass than cisgender women in addition to retaining hand grip strength. Again, we would expect significant inter-individual variability here with larger samples and the extent to which this influences sports performance is not well characterized. Still, this is certainly food for thought when it comes to sports policy.
Unfortunately, that’s the extent of currently published quantitative data on transgender athletes. All the other literature discusses policy, fairness, and other qualitative data. For example, in the 2011 NCAA Policy on Transgender Student-Athletes, Eric Vilain, a physician, professor, and Director of the Center for Gender-Based Biology and Chief Medical Genetics Department of Pediatrics at UCLA, argued:
“Androgen deprivation and cross sex hormone treatment in male-to-female transsexuals reduces muscle mass; accordingly, one year of hormone therapy is an appropriate transitional time before a male-to-female student-athlete competes on a women’s team.” NCAA Inclusion of Transgender Student-Athletes
However, there is still uncertainty regarding the “fairness” aspect of transgender participation in sport, which continues to center around testosterone. Testosterone levels correlate poorly to athletic performance when it comes to within-gender competition – even in women (or men) who have higher than normal endogenous testosterone levels. Karkazis 2012 Bermon 2018 Less is known about the effects of previous exposure to high levels of endogenous testosterone in the case of MTF individuals, or current exposure to exogenous testosterone in the case of FTM individuals. Neither have been well characterized nor fully understood.
Let’s assume that in the case of transgender women, previous exposure to testosterone does confer an advantage and is associated with greater athletic prowess in excess of 3%. –The relevant question then becomes “Is it significant enough to warrant this level of attention and regulation?”
If the end of the previous paragraph was rewritten with “height” or “body weight” instead of “previous exposure to testosterone”, how would that change the discussion? There are numerous examples of cisgender women with exceptional height and/or weight more typically associated with cisgender men, who are very successful athletically. Should they be ineligible to participate in the women’s division because of their more typically “male” height or weight?
Recommendations and Conclusions
While biological differences in sport are fascinating, testosterone levels, chromosomal makeup, or any other physiological parameter may be no more relevant to a gender eligibility policy than any other naturally occurring human characteristic. A few take-home points:
- Effectively regulating sports divisions based on sex using science is impossible. There are no singular or combinations of objective criteria that can define each sex. Prior attempts to govern sports eligibility based on sex using existing testing methods have failed to provide a workable solution based on chromosome composition, physical exam, etc. In other words: we have no way to consistently differentiate male from female and we have never possessed the ability to do so. Gender and sex are not the same thing. Sex is typically assigned at birth based the appearance on appearance of external genitalia and or chromosomal makeup, whereas gender is socially constructed and may vary from culture to culture and/or change over time. However, sex is difficult to dichotomize into two binary divisions because there are a number of different chromosome compositions consistent with either male or female phenotypes. The phrase “biological sex” is meaningless and is ill-advised.
- The gender gap between men and women’s performance in sport is estimated at 10% to 12%.Thibault 2010 This number increases to about 15% for sports requiring a high degree of upper body strength and is much narrower at approximately 5% for ultra-endurance sports. Sandbakk 2017 Nevertheless, the gap remains between 10-12% for sprint events in running, cycling, and swimming. Sports like Olympic weightlifting and powerlifting report a much larger gap of ~40%, but these numbers are likely to be confounded by other variables including a relatively brief history of participation, equity in training/competition opportunities, sociocultural attitudes about women in strength sports, and inequalities at every level of sport. The gender gap in performance is due to all of these factors and it is reductionist (and wrong) to suggest the gap is all about biology (e.g. testosterone).
- The Court of Arbitration in Sport has determined that women athletes, including those with DSD, with elevated endogenous testosterone may have a competitive advantage of 1-3%, but that this is “insufficient to justify a separation in the category of female athletes since many other factors such as nutrition, coaching, other genetic and biological variations have an impact on athletic performance.” CAS 2015 Thus, it could be argued that current precedent for a “fair” advantage in sport via endogenous hormone production in transgender women is 1-3%.
- There are numerous heritable traits that confer significant advantages in sport, independent of sex or gender. Finnish skier, Eero Antero Mäntyranta, and US Volleyball player, Flo Hyman, discussed earlier serve as excellent examples. Additionally, consider that “at least 73 (different) genetic loci have been associated with fitness and performance phenotypes” Rankinen 2002 These genetic factors can produce advantages in excess of the allowable 1-3% competitive advantage deemed to be attributable to endogenous testosterone in hyperandrogenic women and, potentially, greater than the 10-12% performance gap between men and women. At present, there are no sports organizations using any of these criteria to determine participation eligibility, despite their potential to create an “unlevel playing field.”
- Testosterone levels do not appear to reliably correlate to performance in either men or women within the same gender divisions.Karkazis 2012 Additionally, there is substantial overlap between testosterone levels in men and women. Bermon 2017 This suggests using testosterone levels to determine eligibility for sport may be inappropriate. At present, only the IAAF uses testosterone levels to determine eligibility for the women’s division in a handful of track events. There are no testosterone (or other hormone) eligibility requirements for participation in any men’s division for any sport. The CAS has suggested that this may be discriminatory. CAS 2015
- The existing literature on transgender athletes is lacking. There are few quantitative studies published to date. In the case of transgender women, the Harper study found no performance advantage and the Gooren study found that muscle mass levels in transgender women closely approximated muscle mass levels in cisgender women, though the average muscle mass levels of transgender women remained higher. Harper 2015. Gooren 2004 At this time, it is not possible to confidently determine what, if any, competitive advantage exists for transgender athletes under the current IOC rules. Using data that compares men to women to determine policies for transgender athletes may be inappropriate and lead to erroneous conclusions. There are examples where these data are confounded by errors relating to equity in competition, participation, training opportunities, and misrepresentation. Thibault 2010 Capranica 2013 Guillaume 2009 Bermon 2018
- The Olympic Charter encourages inclusion of individuals without discrimination based on race, color, sex, sexual orientation, language, religion, political or other opinion, national or social origin, property, birth, or other status. The rules of sport exist to ensure “fair-play,” but are ultimately arbitrary. Inclusion, however, is not arbitrary and represents a primary aim of the Olympic Charter. Olympic Charter 2018 It is likely that transgender athletes avoid participation in sport due to fear. Sonja 2014 Putting additional restrictions on eligibility for transgender athletes is unlikely to increase participation rates. Those in a position of power should consider themselves obligated to continually review information and policies to ensure equity and equality in sports participation, to the extent that’s possible.
The potential to do harm by restricting participation in sport is real. Women have been denied opportunities to compete and have been subjected to a level of scrutiny completely absent from the men’s divisions. These exclusionary policies pose risks to the health and the enjoyment of life of those subjected to them, particularly those on the edge of socially-accepted gender norms like DSD and transgender athletes. We should be hesitant to further exclude transgender athletes based on undemonstrated harms to competition when real harms to the excluded individuals are already recognized.
I would propose three potential solutions this issue:
1-Assess Gender like Nationality: Given that science cannot reliably determine what makes a woman a woman and a man a man, perhaps we should stop trying. Instead, we could use a process similar to how international sports organizations regulate nationality. Nationality is contentious subject and an “anything goes” policy might result in a situation where athletes are traded between competing nations. Additionally, a person’s nationality is not binary and, like gender and sex, cannot be defined satisfactorily by science. For example, can you imagine trying to describe someone’s “American-ness” and if that met criteria to be an American for competitive purposes?
To address this, a parent organization like the IOC could require individuals to register as a particular gender at a qualifying event, e.g. a national or internationally-sanctioned competition, which would take place across all age divisions as well. Then, once an athlete becomes an adult, he or she would sign an affidavit testifying to his or her gender.
Policies would also have to be in place to cover if an adult wishes to change their gender, similar to the current IOC rules about declaring one’s gender no more frequently than once every four years. This policy has the benefit of being consistent with how science currently views gender and sex without limiting the inclusion of individuals based on arbitrary consensus decisions. Pielke 2016
The appropriate policies for transgender athletes should be tailored for each individual sport based on the specific characteristics of the activity and any potential risks. In contrast, a policy for athletes with DSD can likely be universally applied.
2-Open an Additional Division: Another idea — though one that does not address the inherent problems of regulating gender and sex in sport — could involve the addition of a third division in sports for transgender individuals to participate. The LGBT International Powerlifting Championships introduced the “MX” division for inclusion of transgender and intersex athletes in 2018.Gay Games Website The benefits of this idea are two-fold: 1) Transgender, intersex, and non-binary individuals get to compete in their sport of choice immediately; and 2) Objective data can be collected about performances relative to cisgendered athletes in order to further the discussion about inclusion of transgendered and intersex individuals in conventional sports’ two gender divisions, if desired.
Joanna Harper, who was discussed earlier, has lent some support to this idea.Harper 2018 Additionally, the TUE Chair for the USAPL, Dr. Kris Hunt, as well as long-time USAPL president, Larry Maile, both agreed they were in favor of this idea being proposed at the next committee meeting. Personal Communication Hunt 2019 As described above, this policy may be a viable strategy for some sports and not others when considering transgender individuals in isolation. For example, the risk of harm to other competitors from including transgender women is likely much lower in non-contact sports (e.g. track and field) than in contact sports like boxing or MMA fighting.
On the other hand, implementation of this idea poses substantial drawbacks:
- It fails to address the inherent problems with regulating gender and sex based on science alone.
- It limits participation of trans and intersex individuals in the gender division with which they identify.
- This division would require the transgender athlete to identify themselves as being transgender, which has been shown to limit participation in other activities. Sonja 2014
- If participation is very low, requiring transgender athletes to participate only in their own division may function as a ban from participating at all. Consider if the sport of soccer adopted a transgender woman division, but there weren’t enough players to form multiple teams. The rule would effectively limit participation, not encourage it.
3-Keep Things the Same: Practically speaking, yes, the powers that be could just keep things the same. Sports – and the rules that govern them – are just collections of arbitrary consensus statements that have been collated into a rulebook. With respect to powerlifting, there are over 50 separate federations within the United States, 14 of which have international affiliates, and each functioning autonomously under their own collection of arbitrary consensus statements called rules. As such, sports organizations likely enact policies in order to fulfill their own mission statements and advance the interests of their stakeholders. These sports organizations could continue their current policies if they want, though there are consequences to maintaining the status quo.
For example, the Olympic Charter makes it clear that the practice of sport is a fundamental human right that should be secured without discrimination of any kind. Sports that are recognized by the IOC and aim to uphold the Fundamentals of Olympism set forth in the Olympic Charter, are charged with reviewing their rules and rule-making policies in order to support these aims first and foremost. In cases where a sports organization’s policies and values are directly in conflict with the aims of the Olympic Charter, the organization may need to revise its policies and values to more closely align with the Fundamentals of Olympism. Alternatively, the organization may choose to no longer be recognized as a sport by the IOC and thus, no longer subject to the Olympic Charter’s policies and values.
Additionally, sports “punch above their weight class” with respect to their impacts on society. Consider that the NFL has the largest revenue of any sporting organization in the United States, earning $12 billion in 2015.Kaplan 2015 To put this into perspective, Apple earned about $12 billion every two weeks in the first quarter of 2016.Apple 2016 The entire 2013 revenue of all major US sports (including NASCAR and the NCAA) was about $23 billion, or 0.15% of the total US gross domestic product. Despite this, we give sports a ton of attention, namely via television and social media. In 2015, ESPN was the most-watched channel on television and had 18 of the top 27 most-watched shows.ESPN 2015 On Instagram, Cristiano Ronaldo has the highest number of followers in the world at 173.5 million.Fuentes 2019 Thus, sports – and by extension, sporting organizations – have a responsibility to uphold when it comes to furthering the narrative of equity and equality in both sports and society.Schultz 2012 They can and should move towards greater inclusion and equity through policy.
There is support for increasing transgender athletes’ eligibility to compete with the IOC, USAW, CrossFit, and NCAA all making strides towards inclusion. Arne Ljungqvist, former high jumper, vice chairman of WADA, and chairman of the IOC’s Medical Commission had this to say on trangender athletes in sport:
“Ultimately, the number of transsexual athletes who can successfully compete in open international events is likely to be small, in accord with the estimated incidence of gender dysphoria of one in about every 12,000 men and one in about every 30 000 women. Furthermore, the recommended process for gender reassignment as described is rather arduous.
Finally, individuals who fulfill these criteria will likely be at a relatively advanced age athletically, at least in many sports, though there are notable exceptions—eg, in golf, such as Mianne Bagger who recently qualified and has been competing on the Ladies European Tour after competing in the Swedish Telia Tour in 2004. Inevitably there will be transgendered athletes, such as Renee Richards, who will be competitive at a high level, but most will probably wish to compete only at a masters level or at local and regional events.
The recommendations of the International Olympic Committee are being adopted by various sports governing bodies, such as the US Golf Association and Great Britain’s Ladies Golf Union. We believe that they provide a fair and equitable standard.”Ljungqvist 2005
While I’m sure Ljungqvist was trying to be supportive by making these statements, the policies about transgender eligibility in sport should not be influenced by how many transgender individuals will participate in sport or what level they will compete at. Rather, they should be determined by how sports organizations and their rule-makers integrate complex topics like an athlete’s right to participate and fair play with science and current social values (right or wrong). Finally, policies for DSD and transgender athletes should be considered separately so as not to be conflated.
Executive Summary
Fairness in sport, particularly on the issue of gender, has been a point of confusion and contention for as long as governing bodies have been making the rules for athletic contests. Increasing awareness and visibility of individuals who do not neatly fall into men’s or women’s divisions have exacerbated these concerns. Particular scrutiny has been applied to those who wish to compete as women. Most of the discussion here will focus on that division, since the men’s divisions have been spared this level of examination and controversy.
There has never been a “golden age” when this was simple. In the past, women were simply excluded from sport. As barriers to participation have slowly fallen, questions about who qualifies as a woman for competitive purposes have been raised and unsuccessfully addressed multiple times. Lest an appeal to a more straightforward time be made, we do not, nor have we ever, had an agreed-upon definition of what defines a man or a woman that can be applied to all humans. There is no specific biological characteristic, nor set of characteristics, including genital structures, reproductive organs, or chromosomal arrangement, that can adequately answer this question for this purpose. While most humans can be comfortably grouped into either the men’s or women’s divisions, there are others that cannot. Given that participation in sport is a widely shared and enjoyable undertaking with multiple biological, psychological, and social benefits, finding ways to maximize inclusion while preserving fairness is challenging.
Alas, there are no clear answers. Lacking a consistent way to define men and women hamstrings the proceedings from the outset. When examining the performance differences between men’s and women’s divisions, confounders in the data abound. Teasing out the physiological and psychosocial components of the differences we observe is not yet possible. Even the role of testosterone, which is one of the mostly widely utilized performance enhancing drugs and thought to be the primary arbiter of the gender gap in sports, becomes less clear when looking at the research. Lastly, there is a paucity of research into how athletic performance changes when an individual transitions between genders.
This handwringing is not simply an equivocation. A scientific consensus does not yet exist regarding the differences between genders, let alone how to define those genders. Because of this uncertainty, rules and policies that encourage inclusion of transgender athletes represent the best balance among the imperfect choices available. Specifically, allowing male-to-female transgender athletes to compete in the division of their choice within sport should not be considered prima facie disadvantageous to other women competitors, though this will need to be considered on a sport-by-sport basis. This situation could potentially change or be clarified with further research and we would adjust our recommendations if such findings became available. For now, developing clear and equitable division eligibility policies and subsequently, allowing transgender athletes to compete in the appropriate division is prudent.
Special thanks to Tom Campitelli and Dr. Austin Baraki for their contributions to this article. The article is of much higher quality with their involvement and I am grateful for their time and skills.
References
- IOC Consensus Meeting on Sex Reassignment and Hyperandrogenism November 2015. https://bit.ly/29IcVCv
- Fuentes, Tamara. The 10 Most Followed Celebreties on Instagram. April. 2019. https://bit.ly/2XkZumU
- Shahani S, Braga-Basaria M, Maggio M, Basaria S. Androgens and erythropoiesis: past and present. J Endocrinol Invest. 2009;32(8):704–716
- Van den Tillaar R, Ettema G. Effect of body size and gender in overarm throwing performance. Eur J Appl Physiol 2004;91(4):413-8
- Gender and Genetics. World Health Organization. February 23, 2012. https://www.who.int/genomics/gender/en/index1.html
- NCAA Inclusion of Transgender Student-Athletes 2011. http://www.ncaapublications.com/p-4335-ncaa-inclusion-of-transgender-student- athletes.aspx
- Zaenglein AL, Pathy AL, Schlosser BJ, et al. Guidelines of care for the management of acne vulgaris. J Am Acad Dermatol. 2016; 74(5):945-973.e33.
- Neumann, Friedmund (1996). “Pharmacology of Cyproterone Acetate — A Short Review”. Antiandrogens in Prostate Cancer. pp. 31–44.
- Bermon S, Garnier PY, Hirschberg AL, et al. Serum androgen levels in elite female athletes. J Clin Endocrinol Metab. 2014;99(11):4328-4335
- Factsheet: Women in Leadership Positions within SportAccord Members. Sport-Accord.com. https://bit.ly/30bJcK3
- Schultz, Jaime. New Standards, Same Refrain: The IAAF’s Regulations on Hyperandrogenism, The American Journal of Bioethics, 2012.12:7, 32-33.
- Court of Arbitration for Sport (July 2015). CAS 2014/A/3759 Dutee Chand v. Athletics Federation of India (AFI) & The International Association of Athletics Federations (IAAF) (PDF). Court of Arbitration for Sport.
- Momaya, A., Fawal, M., & Estes, R. (2015). Performance-Enhancing Substances in Sports: A Review of the Literature. Sports Medicine, 45(4), 517–531.
- Heymsfield SB, Gonzalez MC, Lu J, Jia G, Zheng J. Skeletal muscle mass and quality: evolution of modern measurement concepts in the context of sarcopenia. Proc Nutr Soc. 2015 Nov; 74(4):355-66.
- Silventoinen K, Sammalisto S, Perola M, Boomsma DI, Cornes BK, Davis C, Dunkel L, De Lange M, Harris JR, Hjelmborg JV, Luciano M, Martin NG, Mortensen J, Nistico L, Pedersen NL, Skytthe A, Spector TD, Stazi MA, Willemsen G, Kaprio J. Heritability of adult body height: a comparative study of twin cohorts in eight countries. Twin Res. 2003;6(5):399–408.
- Beunen G, Thomis M. Gene powered? Where to go from heritability (h2) in muscle strength and power? Exerc Sport Sci Rev. 2004;32(4):148–154.
- Silventoinen K, Magnusson PK, Tynelius P, Kaprio J, Rasmussen F. Heritability of body size and muscle strength in young adulthood: a study of one million Swedish men. Genet Epidemiol. 2008;32(4):341–349.
- Harper, Joanna. “Race Times for Transgender Athletes.” (2015). https://bit.ly/2LyNQh0
- Courant F, Aksglaede L, Antignac JP, Monteau F, Sorensen K, Andersson AM, Skakkebaek NE, Juul A, Bizec BL. Assessment of circulating sex steroid levels in prepubertal and pubertal boys and girls by a novel ultrasensitive gas chromatography-tandem mass spectrometry method. J Clin Endocrinol Metab. 2010;95(1):82–92.
- Janssen, Ian, Heymsfield, Steven B, Wang, ZiMian, & Ross, Robert. Skeletal muscle mass and distribution in 468 men and women aged 18–88 yr. Journal of Applied Physiology 2000 89:1, 81-88
- Kaplan, Daniel. NFL projecting revenue increase of $1B over 2014. Sports Business Journal, March. 2015. https://bit.ly/2Xj1gox
- Olympic Charter 2018. https://bit.ly/2Yslngv
- Slawinski J, Termoz N, Rabita G, Guilhem G, Dorel S, Morin JB, Samozino P. How 100- m event analyses improve our understanding of world-class men’s and women’s sprint performance. Scand J Med Sci Sports 2017;27(1):45-54.
- Clark, R. V., Wald, J. A., Swerdloff, R. S., Wang, C., Wu, F. C. W., Bowers, L. D., & Matsumoto, A. M. Large Divergence in Testosterone Concentrations between Men and Women: Frame of Reference for Elite Athletes in Sex-Specific Competition in Sports, a Narrative Review. Clinical Endocrinology. 2018.
- Ferguson-Smith MA, Ferris EA. Gender verification in sport: The need for change? Br J Sports Med 1991; 25:17-20.
- IAAF, Regulations Governing Eligibility of Females with Hyperandrogenism. 2018. https://bit.ly/2vOgXGH
- IAAF, Regulations Governing Eligibility of Females with Hyperandrogenism. 2011.https://bit.ly/2J7BUkJ
- Heggie V. Testing sex and gender in sports; reinventing, reimagining and reconstructing histories. Endeavour. 2010;34(4):157–163.
- Kirchengast, Sylvia.Gender Differences in Body Composition from Childhood to Old Age: An Evolutionary Point of View, Journal of Life Sciences, 2010. 2:1,1-10.
- Harper, J., Martinez-Patino, M.-J., Pigozzi, F., & Pitsiladis, Y. (2018). Implications of a Third Gender for Elite Sports. Current Sports Medicine Reports, 17(2).
- T’Sjoen, G., Weyers, S., Taes, Y., Lapauw, B., Toye, K., Goemaere, S., & Kaufman, J.-M. (2009). Prevalence of Low Bone Mass in Relation to Estrogen Treatment and Body Composition in Male-to-Female Transsexual Persons. Journal of Clinical Densitometry, 12(3), 306–313.
- Karkazis K, Jordan-Young R, Davis G, Camporesi S. Out of bounds? A critique of the new policies on hyperandrogenism in elite female athletes [published correction appears in Am J Bioeth. 2012;12(10):56]. Am J Bioeth. 2012;12(7):3–16.
- 2019 CrossFit Rulebook https://games.crossfit.com/rules/open
- 2019 USAPL Transgender Policy. USAPL. 2019. https://www.usapowerlifting.com/transgender-participation-policy/
- Genel, Myron, and Arne Ljungqvist. “Essay: Gender Verification of Female Athletes.” The Lancet, vol. 366, Dec. 2005.
- Kathrine Switzer, “The Girl Who Started It All,” Runner’s World, May 2007, http://kathrineswitzer.com/site/wp-content/uploads/SwitzerStory_RunnersWorld.p df.
- Gallagher, D., Visser, M., De Meersman, R. E., Sepúlveda, D., Baumgartner, R. N., Pierson, R. N.,Heymsfield, S. B. (1997). Appendicular skeletal muscle mass: effects of age, gender, and ethnicity. Journal of Applied Physiology, 83(1), 229–239.
- Factsheet: Women in Leadership Positions within SportAccord Members,” Sport-Accord.com. https://bit.ly/2YyF3iY
- UCSF Transgender Care, Department of Family and Community Medicine, University of California San Francisco. Guidelines for the Primary and Gender-Affirming Care of Transgender and Gender Nonbinary People; 2nd edition. Deutsch MB, ed. June 2016.
- Perez-Gomez J, Rodriguez GV, Ara I, Olmedillas H, Chavarren J,
- Gonzalez-Henriquez JJ, Dorado C, Calbet JA. Role of muscle mass on sprint performance: gender differences? Eur J Appl Physiol 2008;102(6):685-94.
- LGBT INTERNATIONAL POWERLIFTING ANNOUNCES NEW “MX” CATEGORY, Jan 2018.https://gaygames.org/latest-news/5656204
- Mohanty, D.I am who I am: Dutee Chand. The Indian Express, September, 2014.
- Saraswat A, Weinand JD, Safer JD. Evidence supporting the biologic nature of gender identity. Endocr Pract 2015; 21:199.
- Heylens G, De Cuypere G, Zucker KJ, et al. Gender identity disorder in twins: a review of the case report literature. J Sex Med 2012; 9:751.
- Luders E, Sánchez FJ, Tosun D, et al. Increased Cortical Thickness in Male-to-Female Transsexualism. J Behav Brain Sci 2012; 2:357.
- Martin KA, Anderson RR, Chang RJ, et al. Evaluation and Treatment of Hirsutism in Premenopausal Women: An Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 2018; 103:1233.
- Tanner JM, Goldstein H, Whitehouse RH. Standards for children’s height at ages 2-9 years allowing for heights of parents. Arch Dis Child 1970; 45:755.
- Sandbakk, Ø., Solli, G. S., & Holmberg, H.-C. (2018). Sex Differences in World-Record Performance: The Influence of Sport Discipline and Competition Duration. International Journal of Sports Physiology and Performance, 13(1), 2–8.
- Guillaume M., El Helou N., Nassif H., Berthelot G., Len S., et al. Success in Developing Regions: World Records Evolution through a Geopolitical Prism. PLoS ONE, 2009.4(10)
- Handelsman DJ, Hirschberg AL, Bermon S. Circulating Testosterone as the Hormonal Basis of Sex Differences in Athletic Performance. Endocr Rev.;39(5):803–829.
- Capranica, Laura & Piacentini, Maria Francesca & Halson, Shona & Myburgh, Kathryn & Ogasawara, Etsuko & Millard-Stafford, Mindy. (2013). The Gender Gap in Sport Performance: Equity Influences Equality. International journal of sports physiology and performance. 8. 99-103.
- Morales A, Bebb RA, Manjoo P, et al. Diagnosis and management of testosterone deficiency syndrome in men: clinical practice guideline. CMAJ 2015; 187:1369.
- Pielke, Roger. The Edge: The War against Cheating and Corruption in the Cutthroat World of Elite Sports (p. 173). Roaring Forties Press. 2016.Kindle Edition.
- WADA Prohibited List .2019. https://bit.ly/2RDGM3s
- Hunt, K. (2019, June). Phone interview with USAPL Medical Director, Kris Hunt, MD.
- Gentil P, Steele J, Pereira MC, Castanheira RP, Paoli A, Bottaro M. Comparison of upper body strength gains between men and women after 10 weeks of resistance training.PeerJ. 2016;4:e1627, Feb, 2016.
- Longcope C. Adrenal and gonadal androgen secretion in normal females. Clin Endocrinol Metab 1986; 15:213.
- Epstein, David. The Sports Gene: Inside the Science of Extraordinary Athletic Performance (p. 267). Penguin Publishing Group. Kindle Edition.
- Knechtle B, Rosemann T, Lepers R, Rust CA. Women outperform men in ultradistance swimming: the Manhattan Island Marathon Swim from 1983 to 2013. Int J Sports Physiol Perform 2014;9(6):913-24.
- IOC, “Factsheet: Women in the Olympic Movement,” Olympic.org, updated January 2016, https://bit.ly/2J6MBUM
- Redkal,Ole Bjorn, “Academic Urban Legends,” Social Studies of Science 44, no.4(2014):638-654.
- Thibault V, Guillaume M, Berthelot G, et al. Women and Men in Sport Performance: The Gender Gap has not Evolved since 1983. J Sports Sci Med. 2010;9(2):214–223, June, 2010.
- Keierleber, Joseph. How Chromosomes X and Y Got Their Names, 1891. The Scientist. Mar, 2019. https://www.the-scientist.com/foundations/how-chromosomes-x-and-y-got-their-names–1891-65508
- Bermon, S., & Garnier, P.-Y. (2017). Serum androgen levels and their relation to performance in track and field: mass spectrometry results from 2127 observations in male and female elite athletes. British Journal of Sports Medicine, 51(17), 1309–1314.doi:10.1136/bjsports-2017-097792
- Bermon, S., Hirschberg, A. L., Kowalski, J., & Eklund, E. (2018). Serum androgen levels are positively correlated with athletic performance and competition results in elite female athletes. British Journal of Sports Medicine, bjsports–2018–099700. doi:10.1136/bjsports-2018-099700
- Pielke, Robert. A Call for Bermon and Garnier (2017) to be Retracted. The Sports Integrity Initiative. July, 2018. https://www.sportsintegrityinitiative.com/call-bermon-garnier-2017-retracted/
- Rankinen T, Perusse L, Raurama R, Rivera MA, Wolfarth B, Bouchard C (2002) The human gene map for performance and health-related fitness phenotypes: the 2001 update. Med Sci Sports Exerc 34:1219–1233
- About the Sport. Paralympic Powerlifting. 2016. https://www.paralympic.org/powerlifting/about
- World Games Results. International Powerlifting Federation. 2013. https://www.powerlifting.sport/championships/results/world-games-results.html
- Lee PA, Houk CP, Ahmed SF, et al. Consensus statement on management of intersex disorders. International Consensus Conference on Intersex. Pediatrics 2006; 118:e488Blackless M, Charuvastra A, Derryck A, et al. How sexually dimorphic are we? Review and synthesis. Am J Hum Biol 2000; 12:151.
- Dreger, Alice Domurat. 1998. Ambiguous Sex—or Ambivalent Medicine? Ethical Issues in the Treatment of Intersexuality. Hastings Center Report, 28, 3: 24-35.
- Perrin EC. Sexual Orientation in Child and Adolescent Health Care, Springer, New York 2002.
- Hembree WC, Cohen-Kettenis PT, Gooren L, et al. Endocrine treatment of gender-dysphoric/gender-incongruent persons: An Endocrine Society* Clinical Practice Guideline. J Clin Endocrinol Metab 2017.
- Adelson SL, American Academy of Child and Adolescent Psychiatry (AACAP) Committee on Quality Issues (CQI). Practice parameter on gay, lesbian, or bisexual sexual orientation, gender nonconformity, and gender discordance in children and adolescents. J Am Acad Child Adolesc Psychiatry 2012; 51:957.
- Frankowski BL, American Academy of Pediatrics Committee on Adolescence. Sexual orientation and adolescents. Pediatrics 2004; 113:1827.
- Edwards-Leeper L, Spack NP. Psychological evaluation and medical treatment of transgender youth in an interdisciplinary “Gender Management Service” (GeMS) in a major pediatric center. J Homosex 2012; 59:321.
- Rafferty J, Committee on Psychosocial Aspects of Child and Family Health, Committee on Adolescence, Section on Lesbian, Gay, Bisexual, and Transgender Health and Wellness. Ensuring comprehensive care and support for transgender and gender-diverse children and adolescents. Pediatrics 2018; 142:e201821
- Raveenthiran V. Neonatal Sex Assignment in Disorders of Sex Development: A Philosophical Introspection. J Neonatal Surg. 2017;6(3):58. Published 2017 Aug 10. doi:10.21699/jns.v6i3.604
- Short SE, Yang YC, Jenkins TM. Sex, gender, genetics, and health. Am J Public Health. 2013;103 Suppl 1(0 1):S93–S101. doi:10.2105/AJPH.2013.301229
- Winter S, Diamond M, Green J, et al. Transgender people: health at the margins of society. Lancet 2016; 388:390.
- Claes L, Bouman WP, Witcomb GL, et al. Non-suicidal self- injury in trans people: associations with psychological symptoms, victimization, interpersonal functioning and perceived social support. J Sex Med. 2015;12(1):168–79.
- Toomey, R. B., Syvertsen, A. K., & Shramko, M. (2018).Transgender Adolescent Suicide Behavior. Pediatrics, e20174218.doi:10.1542/peds.2017-4218
- Sonja J. Ellis, Jay McNeil & Louis Bailey(2014)Gender, stage of transition and situational avoidance: a UK study of trans people’s experiences, Sexual and Relationship Therapy, 29:3, 351-364, DOI: 1080/14681994.2014.902925
- Global health risks: mortality and burden of disease attributable to selected major risks.World health Organization. 2009. https://www.who.int/healthinfo/global_burden_disease/GlobalHealthRisks_report_full.pdf
- Hepp U, Kraemer B, Schnyder U, et al. Psychiatric comorbidity in gender identity disorder. J Psychosom Res. 2005;58(3):259–61.
- 2018 Physical Activity Guidelines Advisory Committee. 2018 Physical Activity Guidelines Advisory Committee Scientific Report. Washington, DC: U.S. Department of Health and Human Services, 2018.
- International Weightlifting Federation Technical and Competition Rules and Regulations. IWF, 2019. https://www.iwf.net/wp-content/uploads/downloads/2019/02/IWF_TCRR_01012019_v2.pdf
- Miller, A. E. J., MacDougall, J. D., Tarnopolsky, M. A., & Sale, D. G. (1993). Gender differences in strength and muscle fiber characteristics. European Journal of Applied Physiology and Occupational Physiology, 66(3), 254–262.doi:10.1007/bf00235103
- Serrano N, Colenso-Semple LM, Lazauskus KK, et al. Extraordinary fast-twitch fiber abundance in elite weightlifters. PLoS One. 2019;14(3):e0207975. Published 2019 Mar 27. doi:10.1371/journal.pone.0207975
- Hannah et al. (2012) Hannah R, Minshull C, Buckthorpe MW, Folland JP. Explosive neuromuscular performance of males versus females. Experimental Physiology. 2012;97:618–629. doi: 10.1113/expphysiol.2011.063420.
- Abe et al. (2000) Abe T, DeHoyos DV, Pollock ML, Garzarella L. Time course for strength and muscle thickness changes following upper and lower body resistance training in men and women. European Journal of Applied Physiology. 2000;81:174–180. doi: 10.1007/s004210050027
- Yildiz, B. O. (2006). Diagnosis of hyperandrogenism: clinical criteria. Best Practice & Research Clinical Endocrinology & Metabolism, 20(2), 167–176. doi:10.1016/j.beem.2006.02.004
- Gooren, Louis J and Mathijs C Bunck. “Transsexuals and competitive sports.” European journal of endocrinology151 4 (2004): 425-9 .
- Morton RW, Sato K, Gallaugher MPB, et al. Muscle Androgen Receptor Content but Not Systemic Hormones Is Associated With Resistance Training-Induced Skeletal Muscle Hypertrophy in Healthy, Young Men. Front Physiol. 2018;9:1373. Published 2018 Oct 9. doi:10.3389/fphys.2018.01373
- Morton, Robert W. Sara Y. Oikawa, Christopher G. Wavell, Nicole Mazara, Chris McGlory, Joe Quadrilatero, Brittany L. Baechler, Steven K. Baker, and Stuart M. Phillips. Neither load nor systemic hormones determine resistance training-mediated hypertrophy or strength gains in resistance-trained young men Journal of Applied Physiology 2016 121:1, 129-138
-
Muscle strength, size and composition following 12 months of gender-affirming treatment in transgender individuals: retained advantage for the transwomen.