
For an introduction to this program, please check out The Barbell Medicine Podcast: Episode #58: Programming For Beginners (and other musings on training)
You can sign up to download the Beginner Prescription here.
Introduction & Goals
At Barbell Medicine, our mission is to promote health and successful aging by bringing the best of modern medicine together with strength, conditioning, and nutrition. With this document, we want to provide an answer to the question, “Where do I start with exercise to improve my health?”
Health is “the ability to adapt and self-manage in the face of social, physical, and emotional challenges” (Huber 2011). Important here is the concept of self-efficacy, defined as an individual’s belief in their own “capabilities to execute a course of action” or to achieve a goal (McAuley 2011). People who feel they have control over their situations demonstrate greater self-efficacy. Promoting health in a way that comports with this definition requires attention to various biological, psychological, emotional, social, and environmental factors that can influence our health and well-being (Engel 1977). These influences are commonly grouped together and referred to as biopsychosocial factors. One of the most potent interventions available that can improve health through these mechanisms is physical activity.
Physical inactivity is a major health problem worldwide and is the fourth greatest global risk factor for mortality according to the World Health Organization (WHO), behind high blood pressure, tobacco use, and elevated blood sugar (WHO 2009). It predisposes individuals to a wide variety of chronic diseases, including cardio-cerebrovascular disease, metabolic disease, musculoskeletal disorders, frailty, and many others. Unfortunately, low levels of physical activity are endemic in the United States, with only 26% of men, 19% of women, and 20% of adolescents meeting current recommendations for exercise (Piercy 2018).
The authors of the 2018 Physical Activity Guidelines for Americans describe the impact of sedentary behavior, stating:
“… low levels of physical activity among Americans have health and economic consequences for the nation, with nearly $117 billion dollars in annual healthcare costs and 10% of all premature mortality attributable to failure to meet levels of aerobic physical activity recommended in the guidelines.”
These are alarming statistics, but easily-implemented changes have measurable positive effects. Regular participation in physical activity, including resistance training, has well-documented benefits for numerous health outcomes, diseases, and risk of premature death (Kodama 2009 Wescott 2012). For example, taking an additional 2000 steps per day (about 20 minutes of brisk walking) reduces the risk of having a cardiovascular event by 10% and reduces the risk of having elevated blood sugar by 25% (Yates 2014 Ponsonby 2011). With respect to resistance training in particular, there appears to be a 23% reduction in all-cause mortality in individuals who resistance train 2-3 times per week (Dankel 2016), with a “dose-response” relationship between training volume and improvements in health outcomes (Figueiredo 2018). This dose-response relationship is seen when larger doses (of training volume in this case) produce larger effects (improvements in health outcomes). Finally, there is also a strong association between physical strength and the risk for numerous diseases and mortality (Volaklis 2015). In sum: people seem to get sick and die less when they are stronger.
The 2018 Physical Activity Guidelines for Americans recommend the following targets:
- 150 to 300 minutes per week of moderate-intensity aerobic physical activity*⤈, OR;
- 75 to 150 minutes per week of vigorous-intensity aerobic physical activity*⤈, AND;
- Resistance training of moderate or greater intensity involving all major muscle groups on 2 or more days per week.
*Aerobic physical activities of different intensities can be combined in order to meet activity targets.
⤈ Intensity levels are described in the units Metabolic equivalent of Task, or MET. 1 MET is the rate of energy expenditure at rest, whereas a 4 MET activity expends 4 times the energy used by the body at rest. Moderate-intensity activities are defined as 3-5.9 METs, e.g. walking at 3 miles per hour (3.3 METs) , heavy gardening (4 METs) , or cycling at 10 miles per hour (4 METs) Vigorous-intensity activity is defined as 6 METs or greater, e.g. strenuous hiking (6 METs), running at 6 miles per hour (10 METs), or aerobic calisthenics (6-10 METs).
Unfortunately, there appears to be a significant bias against regular participation in resistance training. The 2017 National Health Interview Survey data show that while 53.1% of adults age 18 and over met aerobic physical activity guidelines, only 23.5% met guidelines for both aerobic and muscle-strengthening activities (CDC 2017 [pdf]) There are a number of complex biological, psychological, and social factors that influence individuals’ likelihood of participation in, and adherence to, resistance-based exercise (Rhodes 2017). Among the most powerful of these is individual self-efficacy.
Therefore, we are putting forth an approach that aims to help new trainees improve physical performance, build self-efficacy, and work towards meeting current exercise guidelines for health. Depending on where you’re starting from, the template may not get you all the way there, but it will set you on the right track and help build good habits along the way.
It should be noted that this is purposefully NOT designed with the intent of “sport specialization”, or of getting a trainee as strong as possible, as fast as possible in a select few movements. There is evidence that a more generalized approach early in a training career is associated with better long-term athletic success, and this topic is discussed in more detail in the full text template. We are not concerned with how much weight an individual lifts in their first 12 weeks of training (making this an irrelevant metric for comparison), but rather how much they are lifting years later, or more importantly for non-competitive trainees, whether they are still lifting at all.
Who Is This Program For?
This program is aimed at the following three groups:
- Individuals who are new to exercise and/or resistance training (less than 3-6 months of experience in a formal training program).
- Individuals returning from an extended layoff (more than 4 weeks) from resistance training. We get it: life happens and one missed session sometimes turns into a longer break from the gym. The Beginner Template is a great on-ramp for those who have been out of the gym for awhile.
- Individuals returning from an injury. These folks may have been running one of our rehab templates or working with our rehabilitation coaches. Regardless, if a lifter has been unable to train normally for a substantial period of time (more than 4-6 weeks), they are also a candidate to use this template.
Program Structure
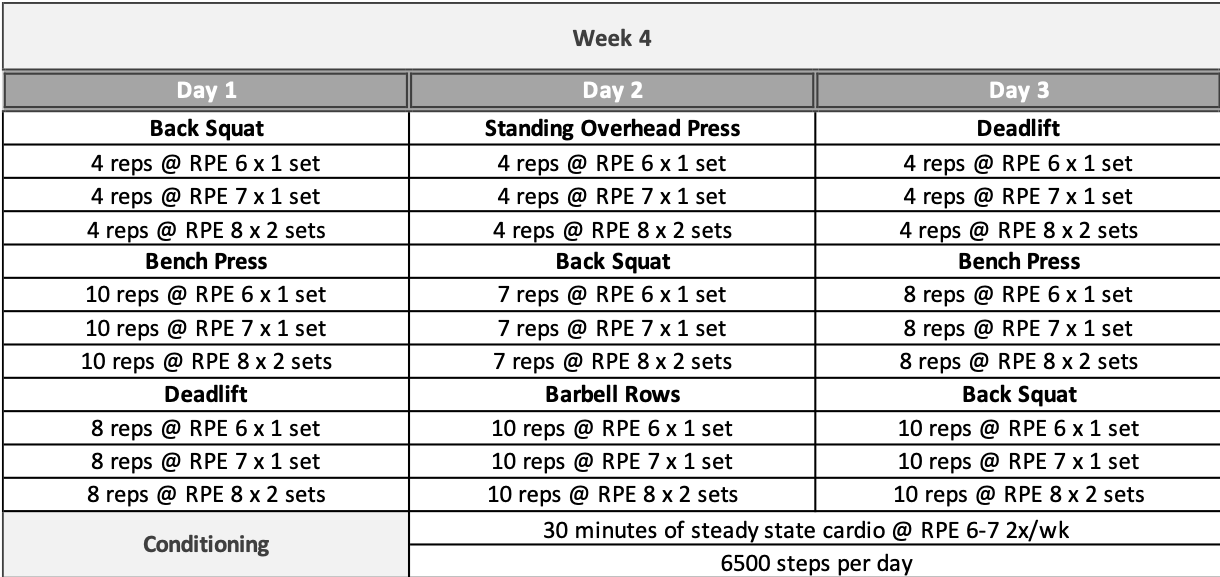
Each week of training includes:
- Three days of strength training involving three exercises per day that collectively train the entire body. These workouts are ideally performed on non-consecutive days (e.g. M/W/F or T/Th/Sa), but if you have to schedule training days back-to-back, that’s okay – and certainly better than not training at all!
- One or two days of conditioning to gradually introduce the trainee to aerobic and anaerobic conditioning elements over time. This serves to improve cardiorespiratory fitness and work capacity for physical development and health outcomes.
This free program is the first of three phases included in the full Beginner Template. The first phase of training begins with the least exercise variation, moderate training intensity, and low training volume that builds over the course of the first four weeks as the individual adapts to the workload. The fourth and final week of this phase is designed to be run repeatedly as long as the trainee is demonstrating a continued trend of improvement. The goals of the first phase are to begin developing:
- technical proficiency with the selected exercises
- proficiency with the use of Ratings of Perceived Exertion [RPE] across a variety of repetition ranges
- work & recovery capacity to improve tolerance for training
Each subsequent phase builds upon the last, with the later phases introducing changes in intensity, rep ranges, training volume, exercise selection, and accessory work. These are designed to produce continued progress in the early phases of a new lifter’s journey, while equipping them with the skills and self-efficacy needed for a successful, long-term training career.
The First Phase
In order to make resistance training more accessible to the general population, the full version of the Beginner Template allows users to select their own exercises from a list of options based on personal preferences, goals, and equipment availability. In the version presented here we will provide pre-programmed defaults that assume the individual is primarily interested in training with barbells. However, for those with equipment limitations or other preferences, these movements can be swapped out for their analogs using machines or other forms of progressive resistance.


HOW TO START
The full template includes a detailed step-by-step set of instructions and explanations walking through the approach to each training session, warming up, selecting loads, and tracking progress. We will provide an abbreviated set of “quick-start” instructions here.
First Workout
Our recommended warm-up involves performing multiple sets of the specific exercise using the empty barbell until you feel mentally and physically prepared to start adding weight. The first session might start like this:
- Squat 4 reps x 1-3 sets (or as many as needed) with the empty barbell (20 kg)
- Squat 4 reps x 1 set with 30 kg
- Squat 4 reps x 1 set with 40 kg
- Squat 4 reps x 1 set with 50 kg (hypothetically RPE 6, first work set)
- Squat 4 reps x 1 set with 55 kg (hypothetically RPE 7, second work set)
- Squat 4 reps x 1 set with 60 kg (hypothetically RPE 8, third work set)
[For instructional videos on the barbell exercises, see the Resources section below.]
Weight Selection
Weights used for each exercise will be selected using Ratings of Perceived Exertion, or RPE. The full text accompanying the Beginner Template contains a more thorough discussion of RPE and a step-by-step guide on how to apply it to select loads for each exercise. For a quick explanation, see the following videos created by Barbell Medicine staff coach Alan Thrall.
Part 1:
Part 2
We understand that introducing this concept to guide loading can be challenging or intimidating for the new Iifter. However, our experience and the current research suggest that most individuals can effectively choose their weights to match a targeted level of exertion within a few weeks to a usable level of accuracy. For some trainees, this may happen much sooner whereas others may take a big longer, which is okay. The use of RPE comes with minimal downsides or risk, especially over the long-term. Again, we are not concerned with the absolute weight lifted in 8-12 weeks, but rather how an individual is doing years later, and developing these skills early is beneficial. We prefer the use of RPE as a way to manage loading and fatigue, since it captures the effects of all biopsychosocial stressors on a trainee’s performance and fatigue state at a given time. It is critical to note that “perfect” accuracy is not required for this metric to be useful.
The Beginner Template provides several weeks of practice at the beginning of each block to help develop a trainee’s skills with estimating and applying RPE to their training across a variety of repetition ranges for a given exercise, as it will become a critical tool as they become more advanced. While we recommend developing the skill of RPE-based autoregulation, if an individual is strongly opposed to its use for load selection, the full template also includes percentage guides for relative intensity targets as well.
Progression
The full template contains a detailed discussion of progression methods and how to monitor your progress over time. The expectation is that, on average, an individual should be getting demonstrably stronger week-to-week when following appropriate programming. With that said, there isn’t a one-size-fits-all answer regarding how much weight to add per week, as individuals vary greatly in their response to a given training program (Ahtiainen 2016). In general, we recommend adding approximately 1-5% per week without overshooting the recommended RPE targets.
It is important to avoid getting emotionally attached to calculated/predicted numbers; as we gather more and more feedback from each set, we can adjust in real time based on actual performance. Of course, life happens, and you may not always be able to add the desired amount in a given session within the parameters of the program, and that’s okay in the short-term. The idea is to assume you’ll be adding weight until/unless proven otherwise based on how you’re actually performing during that training session.
WHAT’S NEXT?
The first phase of the program can be run as described above, with the fourth week being repeated as long as the individual is continuing to demonstrate a trend of improvement (e.g., via estimated 1-rep maximums or other metrics). Once two or more lifts have stalled or regressed for multiple weeks, we recommend moving on from the first phase of the program.
At this point you are in a position to choose what you want to do next depending on your goals. Our recommendation would be to move on to the full version of the Beginner Template to build a larger base of physical development using the second and third phases prior to moving on to more advanced training.
The full template is available HERE.
It contains:
- A 60-page full-text discussion including scientific references about the program’s design, more detailed instructions and descriptions of how to run the program and track progress, as well as explanations of exercise programming with respect to specific health conditions like diabetes, high cholesterol, and several others.
- An Excel template including a training log and analysis tools, RPE chart/calculator, nutrition tracker and additional built-in resources.
Alternatively, you could move on to one of our other templates if you have identified a particular interest like powerlifting, weightlifting, hypertrophy, endurance, etc. — or you may pursue a different training approach entirely.
So if you choose to pursue the full template, we hope you enjoy it. If not, we wish you luck and success with whatever training approach you pursue, and look forward to seeing where you end up in 10 years!
Resources
For technical issues, please send an email to support@barbellmedicine.com
How to Squat
How to perform the Bench Press
How to perform the Standing Overhead Press
How to perform the Deadlift (Conventional; sumo is OK too!)
A Guide to RPE
Part 1:
Part 2:
Tracking Progress Using Estimated 1-rep Maxes
Managing Pain & Injury in the Gym
Recovering From Injury by Charlie Dickson
Nutrition
- To Be a Beast (Where to Start for Nutrition) by Jordan Feigenbaum
- How to Measure Your Waist Correctly by Jordan Feigenbaum
- Barbell Medicine Forum & Training Logs
- Barbell Medicine Facebook Group
Special thanks to Tom Campitelli for his contributions to this article.
References
- Kodama S, Saito K, Tanaka S, et al. Cardiorespiratory fitness as a quantitative predictor of all-cause mortality and cardiovascular events in healthy men and women: a meta-analysis. JAMA 2009; 301:2024.
- Westcott WL. Resistance training is medicine: effects of strength training on health. Curr Sports Med Rep 2012; 11:209
- Volaklis KA, Halle M, Meisinger C. Muscular strength as a strong predictor of mortality: A narrative review. Eur J Intern Med 2015; 26:303.
- Ortega FB, Silventoinen K, Tynelius P, Rasmussen F. Muscular strength in male adolescents and premature death: cohort study of one million participants. BMJ 2012; 345:e7279.
- Ling CH, Taekema D, de Craen AJ, et al. Handgrip strength and mortality in the oldest old population: the Leiden 85-plus study. CMAJ 2010; 182:429.
- Li R, Xia J, Zhang XI, et al. Associations of Muscle Mass and Strength with All-Cause Mortality among US Older Adults. Med Sci Sports Exerc 2018; 50:458.
- National Center for Health Statistics. Early Release of Selected Estimates Based on Data From the 2017 National Health Interview Survey, Centers for Disease Control and Prevention, 19 June 2018.
- Piercy KL, Troiano RP, Ballard RM, et al. The Physical Activity Guidelines for Americans. JAMA.2018;320(19):2020–2028. doi:10.1001/jama.2018.14854
- Engel. The need for a new medical model: a challenge for biomedicine. Science. 1977 Apr 8;196(4286):129-36.
- Huber et al. How should we define health? BMJ 2011;343:d4163
- Ahtiainen et al. Heterogeneity in resistance training-induced muscle strength and mass responses in men and women of different ages. Age (Dordr). 2016 Feb;38(1):10.
- Figueiredo, V. C., de Salles, B. F., & Trajano, G. S. (2017). Volume for Muscle Hypertrophy and Health Outcomes: The Most Effective Variable in Resistance Training. Sports Medicine, 48(3), 499–505.
- Rhodes et al. Factors associated with participation in resistance training: a systematic review. Br J Sports Med. 2017 Oct;51(20):1466-1472.
- McAuley, Edward et al. “Self-efficacy: Implications for Physical Activity, Function, and Functional Limitations in Older Adults.” American journal of lifestyle medicine vol. 5,4 (2011): 10.1177/1559827610392704.
- Yates et al. Association between change in daily ambulatory activity and cardiovascular events in people with impaired glucose tolerance (NAVIGATOR trial): a cohort analysis. Lancet. 2014 Mar 22;383(9922):1059-66.
- Ponsonby et al. “Objectively measured physical activity and the subsequent risk of incident dysglycemia: the Australian Diabetes, Obesity and Lifestyle Study (AusDiab).” Diabetes care vol. 34,7 (2011): 1497-502.