Today we’ll be wrapping up our hip pain series with the familiar topic of osteoarthritis, and summarize some practical take-home points at the end (see previous parts 1 ,2, 3, and 4). For an in-depth discussion on osteoarthritis in general, we have a full-length article here, but this article will focus specifically on the hip. The diagnosis of hip osteoarthritis is fairly broad, as the diagnostic criteria include joint pain, stiffness, and limitations in range of motion. Basically, if your hip feels stiff and painful, you may receive a diagnosis of hip osteoarthritis.
As with other issues we’ve discussed, osteoarthritis of the hip is a common finding on medical imaging like X-rays and MRIs. One study of almost 1000 individuals over the age of 50 found 19.6% of subjects having evidence of hip osteoarthritis, although only 4.2% of this population had hip pain. Kim 2014 This reinforces the idea that “You are not your X-ray”. Outside of imaging tests, most diagnostic criteria involve pain with certain movements (e.g., climbing stairs, squatting, getting into/out of a car) and general weakness of the hip muscles.
However, there are issues with labeling hip pain symptoms as directly and solely attributable to the kinds of structural changes we see on X-rays, since we can’t reverse these changes. Hip and knee osteoarthritis combined have been the 11th leading contributor to disability for the last 30 years worldwide. Cross 2014 Many individuals fear the meaning of this diagnosis, and withdraw from work and other valued life activities as a result of being told they have joint arthritis. Discussing hip osteoarthritis in this way — for example, blaming it on “wear and tear” — does not encourage hope for the improvements that can be achieved through active rehabilitation. So, a more encompassing (if somewhat less satisfying) diagnosis here might just be “hip pain”.
Physical Activity
Addressing hip pain first involves finding the level of activity the person can tolerate and building gradually from there. We have plenty of research showing that exercise is effective for decreasing pain and improving function, but “exercise” is a very general term. Fransen 2014 While many get caught up on what type of exercise is best, we recommend finding any activity an individual can tolerate and building tolerance over time. This reflects the broad range of people experiencing hip pain. Someone who experiences pain with just walking to their mailbox or picking up an object from the ground will have a different starting point than someone who has already been physically active for years and has a recent onset of hip pain. It also requires two entirely different discussions with patients to set appropriate expectations and develop a shared plan.
For individuals with hip pain who are not already physically active, encouraging activities that the person enjoys and can tolerate is paramount. Exercise can include anything that pushes them towards being more active, with no one activity being “best”. The goal is to gradually work towards meeting the physical activity guidelines of 150-300 minutes of moderate–level activity for adults. What constitutes “moderate” is specific to the individual. For people experiencing increased pain who are generally inactive, even low-level activities such as aquatic exercise can be beneficial as a starting point. Bartels 2016
The goals here are two-fold: 1) getting an individual more active, and 2) allowing them to see that they actually can move without flaring up pain symptoms. As the person finds they can tolerate more activity, specific parameters come into play for increasing function and decreasing pain over time.
The emphasis on working towards meeting physical activity recommendations stems from evidence that individuals diagnosed with osteoarthritis tend to be less active in general. de Groot 2008 Behaviors such as being more active and not smoking can have profound effects on staving off chronic diseases as well. Nyberg 2020 While many folks focus on saying certain movements are “bad” or will “wear out” joints, we have far more reason to believe that the type of activity is not nearly as important as continuing to be active. It seems that the only “bad” movement is not moving at all. A 2018 Cochrane review says it best (emphasis ours):
“Chronic hip and knee pain affects all domains of people’s lives. People’s beliefs about chronic pain shape their attitudes and behaviours about how to manage their pain. People are confused about the cause of their pain, and bewildered by its variability and randomness. Without adequate information and advice from healthcare professionals, people do not know what they should and should not do, and, as a consequence, avoid activity for fear of causing harm.” Hurley 2018
It is safe for individuals with hip osteoarthritis to move, and they are not going to “wear out” their joints with exercise. Lots of individuals with X-ray findings of osteoarthritis do not experience pain, and a higher proportion of those are more physically active. Promoting the idea that movement causes harm to the joints encourages people to be less active, which has consequences not only for their joints, but for their general health as well. We must consistently deliver messaging that it is safe to move, and is essential for overall health.
Strength training
Physical activity guidelines also recommend muscle strengthening activities involving the whole body performed on two days per week. These kinds of activities can similarly improve symptoms of osteoarthritis. Zacharias 2014 For individuals with hip pain who are more active but not lifting weights, this should be considered as an entry point. In one study of individuals with knee osteoarthritis, increases in strength of 30-40% were needed in order to see results. Bartholdy 2017 To the trained individual, this might appear to be a very large outcome to achieve. However, consider that if an individual starts with a leg extension exercise using 20 pounds and increases this load to 40 pounds, they have already doubled their strength. The same could be said for an individual who begins with a 15 kg empty barbell on a box squat and works towards 30 kg.
Such activities are safe and effective for improving hip pain and function. Individuals who adhere to programs that meet guidelines for strength training show greater benefit than individuals who do not. Mosgen 2017 A large study from 2015 found evidence to recommend the following criteria for a general strength training program:
- 3 sets of 7-9 reps
- Intensity greater than 50% of 1-rep max strength
- 2-3 minutes rest between sets
- 50+ weeks/year Borde 2015
We are less picky about things like specific repetition ranges or rest period duration, but place very heavy emphasis on consistent exercise — 50+ weeks per year.
Physical fitness and treatment of hip-related pain is a continuous effort. Expectations are often set that treatment only needs to be done for a finite period of time, whether it be a passive intervention like a joint injection, or 6 weeks of physical therapy. These kinds of passive treatments are not supported, and exercise needs to be a continuous, lifelong habit in order to be advantageous.
Older individuals, females, and those with lower social functioning tend to be less physically active when experiencing hip osteoarthritis. Stubbs 2015 To some extent, this is likely related to the messaging sent out by healthcare professionals. Even recommending exercise for an older population may be better framed simply as “movement” rather than calling it “exercise” or “training”. For an individual working two jobs and under increased social stress, piling on more demands of formal exercise may seem overwhelming, but instead having discussions about what they can do with the time, energy, and resources they have available may be a better starting point.
The Athlete
The discussion so far has addressed the general population with hip pain, but what about the athlete who already meets physical activity guidelines, lifts weights multiple times per week, and who still develops hip pain? If imaging tests reveal the presence of osteoarthritis, is it significant in this case? In some cases, maybe — but more often it is another incidental finding, meaning that it was likely present all along while the individual felt well, but it was “found” after someone went looking due to pain symptoms. Things occasionally hurt when training, and modifications may need to be made. This does not inherently mean that an imaging finding of osteoarthritis is the direct cause of pain symptoms, or that a particular exercise is “bad”. Instead, it often means that adjustments need to be made to the training program. This might involve temporary changes to exercise selection, range of motion, loading, training volume, or other program variables.
In these instances, it is often hard to offer specific advice to the individual athlete because a more thorough discussion about training history, current training, and future goals needs to be known in order to find the proper entry point and progression plan. The instances of hip pain that are often diagnosed as FAI syndrome or osteoarthritis are often complex and related to multiple factors. Each athlete will have a different combination of contributing factors, as well as a different starting point where their individual program begins.
To make good recommendations, clinicians and coaches need to know an athlete’s full training history. There are often times where an athlete is going through a period of higher-specificity training (e.g., only competition-style squat, bench press, deadlift) that can increase the risk of symptoms. Here, the addition of exercise variety (such as some of the exercises discussed in previous articles in this series) can be useful for addressing symptoms. In other instances, there may have been a recent inflection point resulting in an increase in overall training volume or intensity. Retooling programming variables is often necessary.
External stressors can also contribute to an athlete’s symptoms. Whether increased demand at work, poor sleep, relationship trouble, or living through a hypothetical pandemic, each can contribute to the overall demand on an athlete. In these instances, it may not necessarily require changes to a program, but strategies to better manage these stressors such as sleep hygiene and social support. It can also involve working to accept that there are going to be periods of higher stress in an athlete’s life and allowing that to factor into training decisions like load selection.
When pain symptoms occur, there is also the factor of internal stress that can sometimes be distilled to “How worried am I about this?” Sometimes when dealing with pain, an athlete can become their own worst enemy. This can be amplified by healthcare professionals or coaches pushing narratives that they are fragile or that joints are being worn out or permanently damaged. It is often beneficial to talk with professionals who understand that X-ray findings are just that, X-ray findings, and need to be interpreted in context. On the other side, there is sometimes the opposite view that progress in the weight room must come at any cost — which is not accurate either. Life is not linear, and neither is progress in the gym. Athletes need to manage those expectations and come to embrace the process of working through symptoms.
Lastly, the duration of symptoms plays a role. Symptoms that have been present for months require a slightly different approach than new-onset pain. In both cases, finding the entry point is crucial but sometimes with the sudden, new-onset issues, “give it a few days’ break” can be perfectly fine advice.
Strength Training After A Total Joint Replacement: A Case Study
There will be individuals who will benefit from joint replacement surgery (known as “total hip arthroplasty”, or THA) with the desire to return to training. Depending upon the surgical technique used, and physician preference, there may be some initial restrictions in what is allowed with training. The initial goals are similar to other procedures in re-gaining range of motion and strength. Once restrictions are lifted, it will be a process to build back to prior levels, but there is no reason an athlete cannot return.
To give a real-world example, we will present a case of an athlete who started training with us starting 12 weeks after surgery. This athlete did have a training history prior to surgery which did allow for a more expanded program early on. Twelve weeks after surgery, this was his initial training program:
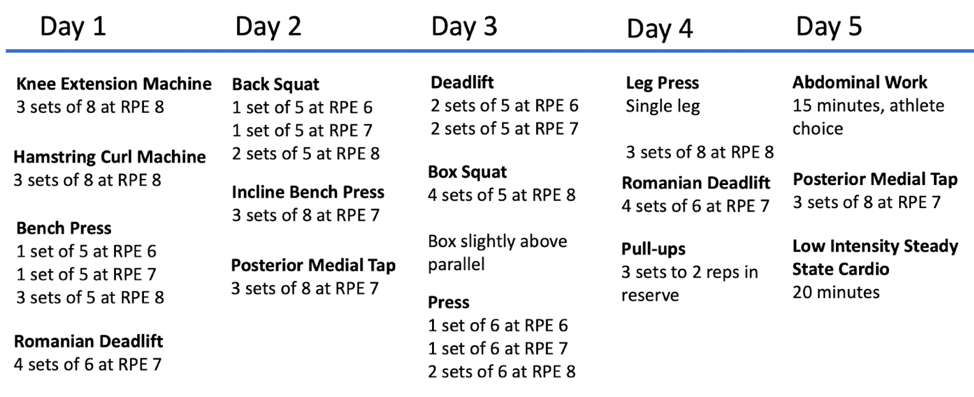
He was able to complete a full body workout, perform isolated strength exercises to get a litmus for any residual strength deficits, and complete some general balance/cardiovascular training. Rate of perceived exertion (RPE) was predicated on more than just effort and was anchored to how his hip felt as well. His first squat is shown below:

There of course are still deficits to address at this point, and every athlete is unique with their starting point in training. What is more important to demonstrate it is possible to both begin training and move weight after a total hip replacement. Three months into training, the program had evolved and the weight on the bar had increased with the program now looking like this:
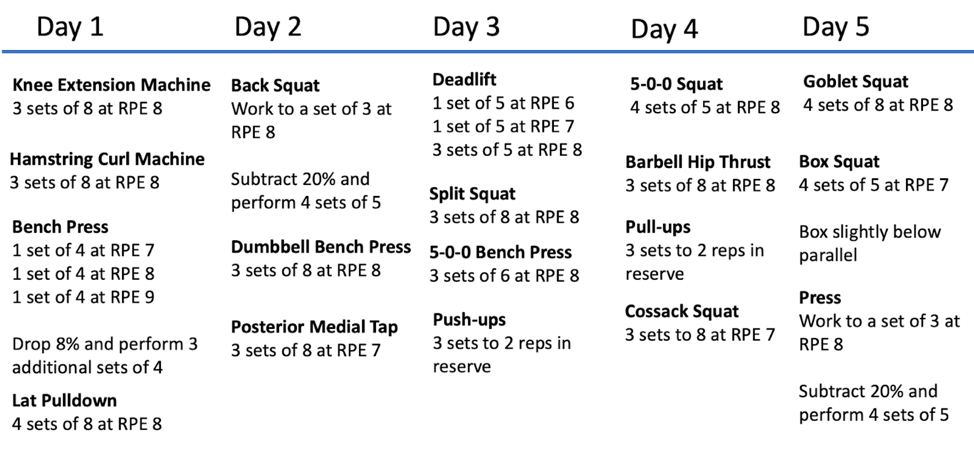
The athlete was also performing other general physical preparation work on a sixth day. He was still not running prior numbers, but as seen in the picture below, there was significant progress in weight on the bar. In instances where an athlete is not quite ready for a program with high intensity, it is possible to spread the work out over more days and add additional variety into the program. The goal is to return to being an “athlete” prior to specializing into a specific type of athlete. Training may involve more single leg work, conditioning, or machine-based exercises, but an athlete can most certainly train.
The selection of exercises will be contingent upon an individual athlete’s goals, but it is paramount that they be treated like an athlete. Many of the exercises offered from traditional rehabilitation programs are of insufficient intensity and volume to elicit meaningful adaptations. This could be said across many different injuries and post-operative scenarios but it is certainly true after joint arthroplasty.
At six months after surgery, this athlete was going to the gym daily, making progress with weight on the bar, and returning to prior levels. As much as specific programming, it was his consistency that allowed for his return. A traditional program that involves bodyweight exercises two times a week for 45 minutes to an hour would not have yielded these results. There are always exercises that an athlete can do and it is the generation of a program within the constraints and limitations of the athlete that will allow them to succeed.
Hip Pain: Summary and Conclusions
This article series is not meant to be comprehensive for the hip, as there are certain instances where further evaluation can be warranted. For example, if an athlete participates in endurance sports and has issues with low nutritional intake, it may raise suspicion for a bone stress injury. These are rare in the lifting community, as one of the benefits of regular resistance training is increased bone density. There are other instances where an athlete may experience numbness around their hip, and these situations should be evaluated by a medical professional. Sometimes though, this is an athlete who is wearing their lifting belt too tight and placing pressure on a superficial nerve much like when your arm falls asleep. Additionally, instances where an athlete is experiencing any problems with bowel or bladder function require further medical evaluation.
For the majority of resistance-trained athletes presenting with hip pain, they will fall into one of three general categories:
- Gradual onset of symptoms, near a tendon. In this case, area-specific work focusing on heavy, SLOW resistance training is beneficial, as well as scaling necessary parts of their program. This may involve substituting different variations of exercises, or it could also necessitate entirely different exercises for a short period. “Heavy” in this context is relative to the individual and their tolerance; if pain spikes significantly during or after training, it should be reduced until the appropriate dose of intensity can be found — and this may be significantly lighter than their “all-time best” strength levels.
- Sudden onset of symptoms, often associated with a sensation of a “pop.” This is typical of a muscle injury. Obvious deformities, especially in the groin, require further medical evaluation. Otherwise, the athlete needs to find ways to move while symptoms begin to subside. It is often advantageous to initially work on different exercises early on, versus using the same movement that precipitated the original injury. From there, direct work on the specific muscle (or group) that was injured is warranted. The current research supports exercises such as the Nordic hamstring curl or Copenhagen adductor exercise for their targeted muscles. However, it is likely that the type of exercise matters more than the specific exercise chosen. Movements using a large range of motion with an emphasis on the eccentric portion are likely to be just as advantageous for building back to prior levels. It is also important to assess strength of the injured muscle as the athlete returns to higher intensity activities. The overall goal for return to competition is greater than 90% symmetry, although this is not to say that an athlete cannot train otherwise. If the athlete is participating in high-speed running, it is also imperative to introduce some speed work prior to returning to full training volume.
- Gradual onset of pain in the front of the hip. To address these issues, the athlete often benefits from modifying training to work on different stances (e.g., switching to sumo-stance, manipulating squat stance and toe/knee angle), exercise variation, and range of motion so that they can better tolerate movement in training. The goal is to slowly increase the capacity for loading in terms of range of motion and intensity as the athlete returns to prior levels of function.
The emergence of pain symptoms in the hip often arises due to multiple factors, and there is no “one weird trick” that all athletes need to perform to become bulletproof. People should be working towards meeting physical activity guidelines, although the specific exercises used to get there are less important; there is no “best” exercise for the general population.
For athletes participating in the strength sports, the emergence of symptoms often means they temporarily need to do something different. It may be variations of their common exercises, or totally different exercises altogether. Changes in anatomical structure may contribute to the emergence of symptoms, but it is important to remember that those changes may also represent adaptations arising from practice in their respective sport. It is not about making all athletes the same, but rather facilitating means where each can succeed in the demands of their respective sports.
If you are having difficulty as an athlete training with hip related issues, you can reach out to the Pain and Rehabilitation Team for consultation and programming to help return to prior levels.